

Why So Many People Told Me To Kill Myself This Weekend
I’m fine, but it was very unpleasant!

It’s been a while since I last burdened this newsletter with a Twitter story. Alas, this is significantly darker than my last one, from February. During the final section, I go into some detail about online suicide-baiting — I’ll clearly mark that section and if you don’t want to see this sort of thing, you should simply skip it.
In one sense, everything that follows is my fault. I did something very stupid: I tweeted. There was no need for me to tweet. There hasn’t been a need for me to tweet for quite some time. I was off Twitter for a couple months this spring and it appeared to have no impact on my ability to grow this newsletter and Blocked and Reported (no, I am not calling Twitter “X” — come on). Not only that, but I was at a Substack event back in New York recently and an engineer there told me that Twitter has basically no effect on paid subscriptions. He said that yes, it brings some people to your newsletter or podcast, but they stick around for six seconds and then flutter off, moth-like, to something else. In neither my experience nor this engineer’s experience does Twitter have much of an impact on paid subscription products. That was the only remaining justification for me to be active on Twitter despite its present state and increasingly disturbed denizens, so there’s really no good reason for me to tweet.
And yet tweet I do. So keep that in mind as you’re reading what follows: even when I’m complaining about other people’s behavior, I could have very easily avoided all of this by doing. . . nothing. By not tweeting. I’m not into self-help but I do think “Sometimes you would have been better off doing nothing rather than what you did” is a very important lesson to internalize. It definitely applies here.
So what did I do instead of “nothing”? On Thursday, I screenshotted part of the transcript of a podcast hosted by Imara Jones called The Anti-Trans Hate Machine: A Plot Against Equality. The podcast is. . . about what you’d expect, given the title. Let’s set that aside. The episode in question features interviews with a young trans woman and activist, Cam Ogden, and her mother, Jeanne Ogden. Jeanne expresses remorse that she made Cam wait so long to go on hormones, stonewalling Cam until she was an adult and could get them herself. The podcast argues that a major reason certain parents are skeptical of their kids transitioning, and in some cases pin their desire to do so on “social contagion,” is a website called 4thWaveNow that is skeptical of youth transition, and that my 2018 Atlantic article played a major role in spreading this idea to the masses. I obviously disagree with all of this, but that isn’t all that relevant to this post, so I’ll stick my response in a footnote for the curious.1
The segment I screenshot suggested Cam had gone through a really shoddy assessment before being approved to start blockers and/or hormones (I guess technically at age 15, blockers followed by hormones would have likely been the path, but the episode is slightly unclear on this, so I’ll continue just saying “hormones” for short):
Here’s the bit from the transcript I included in my tweet, in text form
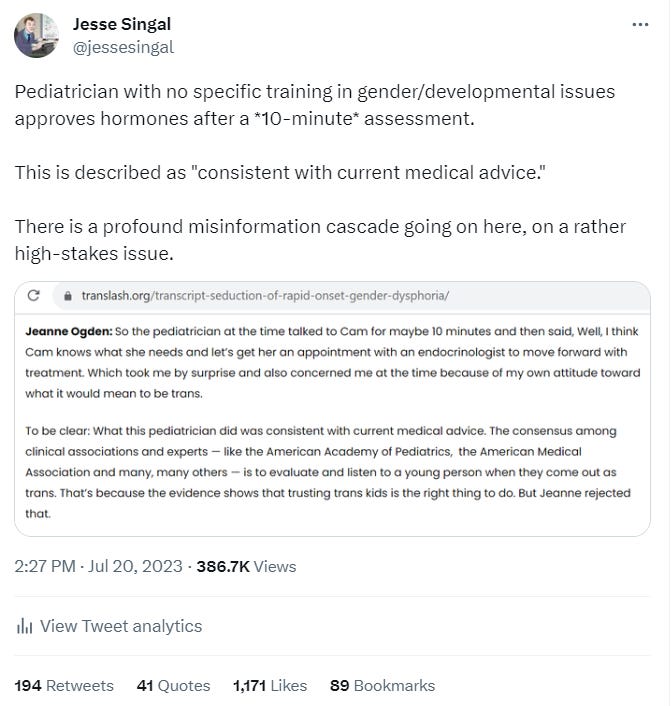
Jeanne Ogden: So the pediatrician at the time talked to Cam for maybe 10 minutes and then said, Well, I think Cam knows what she needs and let’s get her an appointment with an endocrinologist to move forward with treatment. Which took me by surprise and also concerned me at the time because of my own attitude toward what it would mean to be trans.
[Imara Jones:] To be clear: What this pediatrician did was consistent with current medical advice. The consensus among clinical associations and experts — like the American Academy of Pediatrics, the American Medical Association and many, many others — is to evaluate and listen to a young person when they come out as trans. That’s because the evidence shows that trusting trans kids is the right thing to do. But Jeanne rejected that.
Now, in the context of youth gender medicine, “the evidence shows that trusting trans kids is the right thing to do” is a severe oversimplification. What little evidence we have suggesting some kids might benefit from youth gender medicine comes from studies that in fact involved a significant degree of adult diagnosis and gatekeeping. But even setting that aside, this struck me as nuts on multiple levels. First, 10 minutes is obviously not enough time for a doctor to determine that it’s time to “move forward with treatment.” It’s bad enough to present the mom’s skepticism of this perfunctory assessment as anti-trans. It’s even worse for Jones to then claim that this is normal and adheres to professional standards for youth gender medicine. So that’s what I said above the screenshot: “Pediatrician with no specific training in gender/development issues approves hormones after a *10-minute* assessment. This is described as ‘consistent with current medical advice.’ There is a profound misinformation cascade going on here, on a rather high-stakes issue.”
I’m not making this issue up! Anyone who follows the youth gender medicine debate knows that the quality of assessment kids get before beginning treatment is hotly debated, as is — increasingly and rather remarkably — the question of whether assessment is even necessary(!). In an important Washington Post column from November 2021, the psychologists Laura Edwards-Leeper and Erica Anderson, both of whom have sterling credentials treating trans kids (I’ve interviewed them at length, in this article, here, and here), wrote:
When working in gender clinics, we’ve also both received letters from therapists who had “assessed” patients they were referring to us. An astonishing number of these were nothing but a paragraph that stated the youth identified as trans, had dysphoria and wanted hormones, so that course was recommended. There are nearly 200,000 members of the American Psychological Association and the American Psychiatric Association. Add to that the clinical social workers, marriage counselors and family therapists. The overwhelming majority of those well-intentioned professionals receive limited or no training in the assessment of gender-diverse youth. (We receive requests frequently from people eager for more comprehensive, nuanced trainings, which we both deliver.) In simple terms, the demand for competent care has outstripped the supply of competent providers.
In professional circles, we hear from pediatric endocrinologists and others who prescribe hormones for trans youth. Many openly discuss how they use the adult informed-consent model of care with their teen patients, which almost always means no mental health involvement and sometimes no parent input, either. “If you are trans, I believe you,” says A.J. Eckert, the medical director of Anchor Health Initiative in Connecticut. Eckert is wary of psychologists who follow the guidelines by completing a comprehensive assessment before recommending medical intervention for youths. “Gender-affirming medicine,” Eckert holds, means that “you are best equipped to make decisions about your own body,” full stop. These providers do not always realize they’ve confessed to ignoring the standards of care. (Contacted by The Post for comment on this essay, Eckert said that “no medical or surgical interventions are provided to anyone who has not started puberty” but added that, as Anchor Health sees it, “Therapy is not a requirement in this approach because being trans is not a pathology.”)
So of course that’s what I thought of when I read about a pediatrician approving a kid for hormones after 10 minutes. This is the sort of thing that happens. (An incident like this is also one of Jamie Reed’s key accusations about the quality of care at the St. Louis clinic where she turned whistleblower.)
But I’ve made this point before, at length. Why did I tweet about it? What did I hope to gain from pointing this out for the hundredth time? I think it was partially a form of narcissism. From what I’d heard of a different episode of The Anti-Trans Hate Machine: A Plot Against Equality, the show had gone after me in a way I found unfair and unjournalistic. I’d spent a chunk of Tuesday frustratingly tweeting about that. So I guess the road my deeply broken brain led me down was: Why not check out the podcast’s other episodes? Maybe there will be other stuff there you can also get mad about? So I did and there was. What I’m saying is this was all so, so pointless. Pointless and easily avoidable.
At some point not long after my tweet, Cam Ogden herself popped up and accused me of lying about her situation: “Jesse is lying to his audience about my healthcare. He’s using an excerpt from an interview my mother and I did to imply I was fast-tracked into transition, AND accusing TranslashMedia of misrepresenting the SOC by conflating a REFERRAL to a clinic with APPROVAL for HRT.”
Her thread continued:
Both points are false. First, Singal implies Translash supports prescribing HRT after a ten-minute meeting. This is obviously untrue. The text he screenshotted says listening to trans youth when they assert themselves is the accepted standard. . . which is what my doctor did. Next, let’s look at the quote Jesse is taking out of context: A substantial amount of time passed between coming out to my mom and that doctor’s visit. I actually had been seeing a therapist for years, and the doctor had those notes indicating my experience with dysphoria. During those *months of waiting* I met two separate psychologists and spoke to them about dysphoria. There aren’t details in the interview about that because it was traumatic, but if Singal wanted to ACTUALLY hear about my experiences he could have asked me. . . DM’s are still open. I wasn’t “approved for hormones” as Singal claims. I was referred to THRIVE [a gender clinic based at Nationwide Children’s Hospital in Columbus Ohio, link added by me] for an *informational session and evaluation* at their endocrinology clinic. A majority of patients at these clinics don’t receive HRT.
I want to respond to this because it did kick off everything that followed. But for the love of all that is holy, DO NOT BOTHER CAM HERSELF about any of this. Seriously. If you do, you are missing my point entirely and I will be mad and will block you from anything I can block you from. I’m happy to discuss this with her further if she wants to, but 1) there’s obviously no obligation, and 2) I’m avoiding further back and forth about this on Twitter, for reasons that will soon become clear.
Simply put, there are major, important differences between how the podcast described Cam’s experiences and how Cam did in response to my tweet, and if the podcast had included the details Cam subsequently revealed, there would have been no grounds to critique her pediatrician’s actions.
But the podcast painted a seemingly clear picture of what had happened. Cam’s mom simply said: “So the pediatrician at the time talked to Cam for maybe 10 minutes and then said, Well, I think Cam knows what she needs and let’s get her an appointment with an endocrinologist to move forward with treatment.” This is absolutely phrased in a way to suggest the pediatrician approved putting Cam on hormones, and sent her to an endocrinologist with this recommendation in hand.
It’s impossible to say what would have happened then, but of course an endocrinologist is not qualified to conduct any sort of mental health assessment him- or herself, and may well just defer to the referring clinician’s recommendation. Plus, as Edwards-Leeper and Anderson noted, some pediatric endocrinologists are opposed, ideologically, to providing any gatekeeping at this stage. So it isn’t as though the idea of an endocrinologist putting a kid on hormones despite the lack of much assessment is some sort of right-wing fantasy — rather, it’s an ongoing concern among those who are concerned about the quality of care youth gender medicine provides to its patients.
And as described, this was a situation where Cam received no real assessment before being sent to an endocrinologist to start hormones. Further supporting this interpretation is the mom’s response: “Which took me by surprise and also concerned me at the time because of my own attitude toward what it would mean to be trans.” On its face, it makes a lot less sense that she’d be surprised by a recommendation for her kid to be seen for further evaluation than it does that she’d be surprised by a recommendation for her kid to go ahead and start hormones.
From where I sit, the phrase “move forward with treatment” could not be less ambiguous. Not “move forward with further assessment,” not “move forward to meet with a multidisciplinary team” — move forward with treatment. There’s also no mention in the podcast of the fact that the pediatrician was informed that Cam had already discussed her gender dysphoria with not one but two therapists. (The podcast does contain a fleeting reference to therapy, but it occurs right after the mention of the pediatrician, and Imara Jones frames it as part of Cam’s mom’s stonewalling effort, rather than actual work to diagnose and understand her GD: “Jeanne doubled down on her strategy to keep Cam from transitioning. Not only by seeing doctor after doctor and therapist after therapist. But there were also medical professionals who she resisted seeing.”)
Imagine if The Anti-Trans Hate Machine: A Plot Against Equality had included these details, saying something like: “So the pediatrician at the time talked to Cam for maybe 10 minutes, and looked over the notes Cam’s therapists had sent along about her gender dysphoria. The pediatrician then suggested Cam go to THRIVE, a local gender clinic based out of Nationwide Children’s Hospital in Columbus, where she could talk to an endocrinologist, a psychologist, and other experts about potentially starting hormones.” I never, ever would have tweeted anything negative about this — this is a perfectly responsible approach to evaluating kids for youth gender medicine!
THRIVE, by the way, is where the psychiatrist Scott Leibowitz serves as medical director. He’s firmly in the “yes, comprehensive assessment is important” camp, co-led the development of the adolescent section of the latest World Professional Association for Transgender Health Standards of Care, and was featured prominently in my Atlantic story as well as, somewhat randomly, in my last interminable Twitter tale. I visited his clinic for my Atlantic article (like plenty of other stuff, that didn’t make it into the final piece), and I didn’t and don’t get the sense that kids who show up there are going to get the lazy, perfunctory assessment some critics of youth gender medicine are concerned about. So again: with the full facts in hand, there’s nothing obviously suspect about the quality of the assessment Cam would have received had her mom not roadblocked that process. It’s just that none of this was in the actual podcast!
On the one hand, I absolutely disagree with Cam’s claim that I lied or that I needed to reach out before responding to a publicly aired podcast. I thought that, as phrased, the segment was rather unambiguous about what happened. All the further details, which cast things in a very different context, came not from the podcast but from Cam herself, on Twitter, long after the podcast aired. I also disagree with the idea that I was being sneaky or dishonest in describing the podcast’s presentation of the facts as “misinformation” about the prevailing standards of care. Again: as presented, without Cam’s follow-up information, it absolutely reads and sounds as though Imara Jones is saying that a 10-minute evaluation and approval of hormones on the part of a pediatrician follows those standards. I’ve read and reread and reread that section, and I’d be lying if I said otherwise. I do not think my initial interpretation was unwarranted.
On the other hand, again, why tweet about this? I’ve made these points before, often in longer-form venues that allow for much more nuance and much less potential for pointless and social-media drama.The downsides of tweeting about something like this outweigh the upsides by such a wide margin. Maybe, if I’m lucky, the tweet catches on and the people who already agree comprehensive assessments are important and frequently overlooked. . . retweet it? And then what? I gain followers? Between five and seven microunits of clout? The downside — and it’s always the downside in the game of Russian roulette that is tweeting about controversial subjects — is that people get really, really mad about it. At which point you need to explain yourself, at which point you’ve already lost.
Sure enough, Cam’s tweetstorm led to a bunch of Twitter pundits, including some established journalists, expressing outrage at the sheer irresponsibility of my tweet. This proved what they’d been saying all along about how awful a journalist I am (just like my incompetence had been definitively proven in February, during The Great Kale Incident, until all of a sudden it hadn’t been). Many took her claim that I had lied at face value and began disseminating it, and almost immediately that narrative took hold: I had lied, intentionally, about a young trans person’s healthcare, solely to advance my deranged and bigoted agenda. “This thread should be the end of Jesse Singal’s zombie career,” wrote Tabatha Southey, a Canadian writer and former Globe and Mail columnist, in one representative example. “I’m going to say it one more time: Stop hiring Jesse Singal to write anything, you’re neither of you going to come out of it looking smart.”
I was relatively late in responding because I’m in Berlin at the moment, but when I woke up the next day and saw the outrage, I deleted my tweet and posted an explanation that starts here, pointing out that I was relying strictly on how the podcast had presented Cam’s story, not the information she later provided. The penultimate tweet directed readers to Cam’s tweetstorm so they could read her account for themselves.
Naturally, the folks who were already mad used this as an excuse to get madder — they saw my deletion and update as only further proof I’d engaged in a terrible act of journalistic malfeasance. They were also mad at me for blaming the podcast’s lack of clarity rather than looking inward, which, well, I’m not sure what to tell them. I am blaming the podcast’s lack of clarity. Anyone who reads or listens to my work knows that when I actually need to correct something, in the somewhat formal journalistic sense, I do. This is not one of those instances. But of course I didn’t want my original version of events to continue to spread now that Cam had provided much more information; hence the deletion and followup explanation.
None of the outrage which ensued would have normally been worthy of a Singal-Minded post. If I devoted any of this space to 99.9% of the Twitter screeching I experience, the newsletter would quickly become unreadable and my audience would melt away. But this time around was different because of a tweet from Noah Kulwin, a pretty successful, well-known name in lefty media circles: he’s a columnist at Defector, the Deadspin spiritual successor where a lot of Gawker refugees landed, as well as a contributing editor at Jewish Currents, and the cohost of a successful podcast called Blowback (I listened to and enjoyed the first season).
(All right, the suicide stuff starts here, so skip the rest of the post if you don’t want to read it.)
Kulwin’s response to my supposed error — I interpreted a doctor’s recommendation to “move forward with treatment” as. . . a doctor’s recommendation to move forward with treatment — was to tell me I should kill myself:
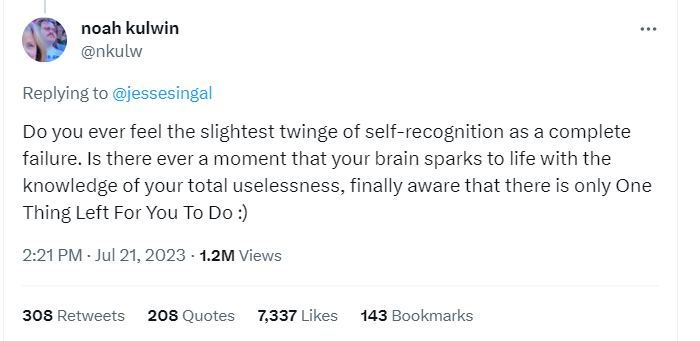
He wrote: “Do you ever feel the slightest twinge of self-recognition as a complete failure. Is there ever a moment that your brain sparks to life with the knowledge of your total uselessness, finally aware that there is only One Thing Left For You To Do :) ” Anyone who speaks internet knows exactly what this means. (The origin of the phrasing is a letter J. Edgar Hoover’s F.B.I. sent to Martin Luther King Jr., trying to get him to kill himself.)
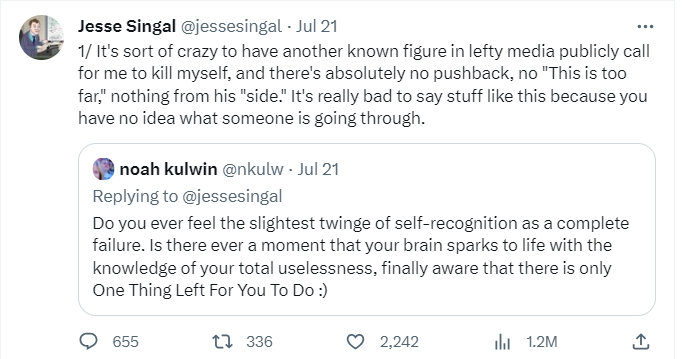
I’m pretty inured to internet madness at this point, but I’ll admit that this disturbed me. Kulwin isn’t some random internet nobody — he’s an established voice in lefty media who works for fairly well-known outlets. I thought that this was inappropriate and said so: “It’s sort of crazy to have another known figure in lefty media publicly call for me to kill myself, and there’s absolutely no pushback, no ‘This is too far,’ nothing from his ‘side.’ It’s really bad to say stuff like this because you have no idea what someone is going through.”
Of course quote-retweeting it made things worse. A large number of people started tweeting at me that yes, I should kill myself. Others expressed searing outrage that I was mad about Kulwin’s tweet given all the blood I have on my hands as a result of my having written that youth gender medicine can help some kids, but that there are holes in the research and comprehensive assessments are important.

In light of the magnitude of my crimes, the absolute least anyone could do was wish for me to end my own life, and I was being such a whiny baby by complaining about an act as self-evidently righteous as Kulwin’s.
As the wave of suicide-bating crested, other journalists in Kulwin’s immediate circle began feverishly doing everything they could to prove me right: there’d be absolutely no pushback to what he had tweeted. Rather than delete the tweet or apologize, Kulwin kept joking about it, at one point claiming that what he’d meant was I should enter therapy.
To which Emma Vigeland, cohost of the big-time lefty talk show and podcast Majority Report tweeted (archive) “Self care king, don’t listen to the noise 🫶”

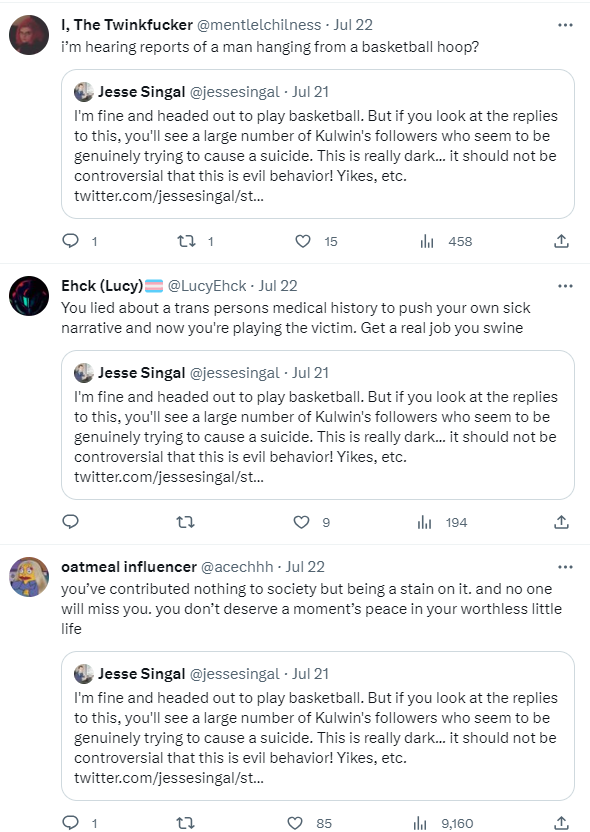
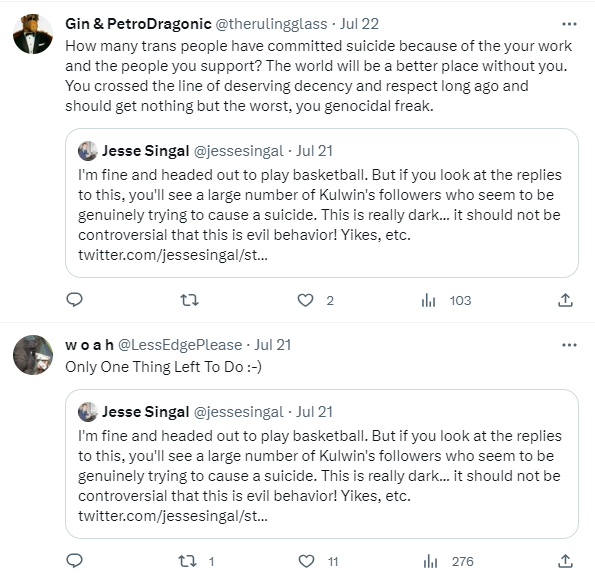
All this happened shortly before I was supposed to leave to go play basketball. I tweeted that I was heading out, simply because I didn’t want to post about disturbing suicide-baiting and then disappear from Twitter (I keep it off my phone), which might worry some people. To make sure the spotlight stayed on me — to make sure more people told me to kill myself — Kulwin quote-retweeted my basketball tweet and said (archive) “Theyre calling it the worlds longest basketball game.”
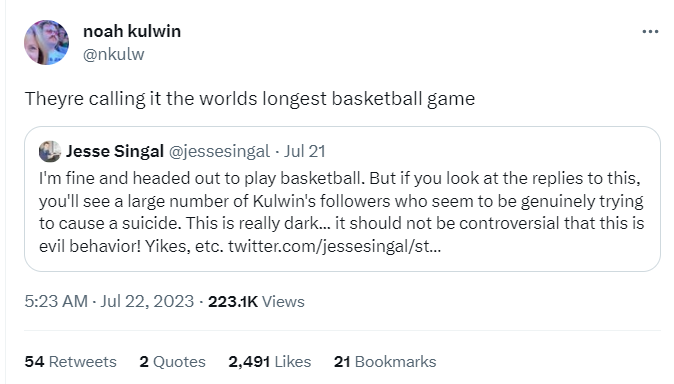
I’m not sure whether Kulwin’s joke here is simply that he had successfully gotten me to log off for a presumably long period of time, or that while I was out, I’d kill myself. Either way, a truly stirring victory for trans rights.
Some Defector staffers joined in on the fun. Tom Ley, the site’s editor-in-chief, responded by saying (archive): “I know we’re pals Noah but I have to agree with Jesse here. You should have been more civil and dug into his medical history in order to make some dogbrained and incorrect observation while publicly humiliating him in the process.” In this view, by screenshotting and responding to a publicly posted podcast transcript, I had “publicly humiliated” Cam and “dug into [her] medical history.” Does this make any sense? Is it at all a faithful description of what had happened? You’d be a sucker for even asking those questions. The whole point here was simply to cast what I did in as grotesque and exaggerated a light as possible so as to justify the suicide baiting and incite more of it.
Kulwin responded (archive): “Wait. . . did he recently do something *exactly* like that? Might this all be some contrived attempt to direct attention elsewhere. . . . Will need to look into this.”

So Kulwin’s take was that I wasn’t actually disturbed by his call for me to kill myself— rather, by complaining about it, I was engaging in a bad-faith ploy to deflect people’s attention from my super-embarassing, privacy-violating (!) error.
David Roth, also an editor at Defector, joined in the fray as well. Having seen his colleague’s original tweet, and having seen me tell everyone I was okay and headed out to play basketball, but that I thought it was inappropriate for a fellow journalist to try to get me to kill myself, Roth responded (archive), “Winner stays on the floor and Jesse is absolutely a PROBLEM.”

To be clear, I think it’s unlikely that in their spare time, Tom Ley or David Roth go around trying to get people to kill themselves (Kulwin, I gotta admit — not so sure. I just get different vibes from his Twitter persona than from theirs). I think the problem here is that they are cowards. They couldn’t clear the lowest moral bar imaginable: gently tell a colleague, maybe via DM so as to not add to the spectacle, “Hey man — we all hate Jesse, what a piece of shit, but maybe lay off the suicide stuff.” Instead, they joined in at a time when, being veterans of the internet, they knew that I was Twitter’s main character of the day, and that every new tweet about me was only going to cause their followers to join in and push things in an uglier and uglier direction.
I guess from their perspective, the whole thing was funny. We might have to agree to disagree on that. From my point of view, if a bunch of people told a journalist to kill himself, and then he did, that would be quite sad. It wouldn’t matter to me if I disagreed with the journalist, even on issues I viewed as important.
Either way, it’s particularly hard to find any of this funny when you’re on the receiving end of it. Here’s a very small taste of what I got from folks who I believe are Kulwin’s followers, based on a couple very rudimentary searches/perusals of replies:
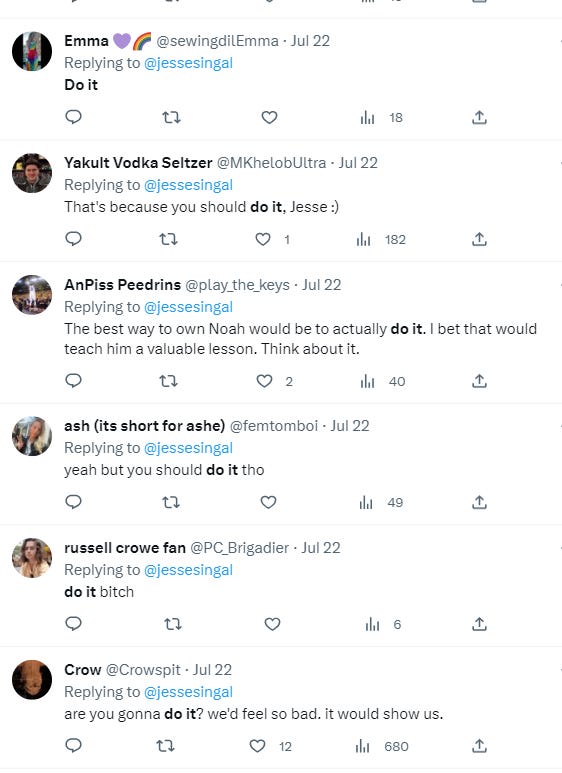

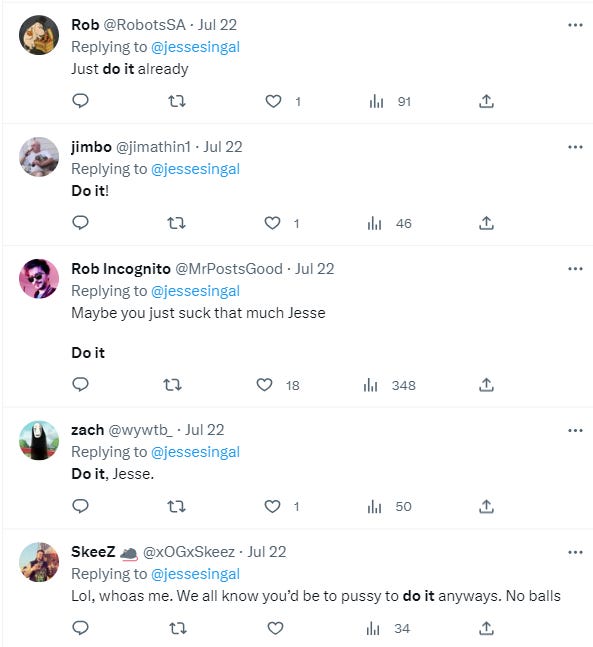

Again: I could have avoided all of this by tweeting less. And of course, Twitter being Twitter, when I complained about it, that was going to exacerbate things. A lot of these people seem to be very, very unwell, and I’m choosing to put myself in close proximity to them. That’s why I don’t view it as newsworthy when random idiots on Twitter yell at me.
But random idiots on Twitter take their cues from the big accounts they follow. So I do think professional journalists, even ones whose professional identities and incomes rely on nihilistic irony, should consider whether suicide-baiting, or encouraging their unwell followers to suicide-bait, is right. Or, if they think it is right, they should consider whether it’s smart. Maybe the next time you tell someone to kill themself and joke about it over and over again as an online crowd forms to cheer you on, you roll snake eyes and it happens to be someone who is in crisis. What happens to you and your career when the most newsworthy thing about their suicide is that it immediately followed you telling them to do it?
I’m completely fine — my being fine was never really in doubt — but of course I found this quite disturbing and different from the other Twitter pileons I’ve experience over the years. How can it not affect you, a bit, to see more than seven thousand people like a tweet calling on you to kill yourself?
As always, if any members of the extended Gawker diaspora want to have a conversation about my actual beliefs on these issues, I’m all ears. Between our respective platforms, there’s no shortage of podcasts where such a conversation could be hosted, and these guys have been taking escalating potshots at me for years, so one would think they’d want an opportunity to show everyone just how wrong and evil I am.
But actually acknowledging uncertainty and hashing out disagreement isn’t the Gawker style. Rather, the Gawker style is an unholy throuple of preening sanctimony, rabid incuriosity, and performative cruelty. It’s a style that couldn’t survive five minutes of actual conversation; in fact, the only sort of place it can not only survive but thrive is on a psychotic medium like Twitter.
And I keep choosing to go back there!
Questions? Comments? Awesome jokes about people killing themselves? I’m at singalminded@gmail.com or on Twitter at @jessesingal.
I’m not going to fully relitigate this, but, briefly and safely tucked away down here: I found the podcast ridiculous. My article couldn’t have been clearer in its support for well-assessed kids going getting youth gender medicine, and it highlighted specific kids who appeared to have benefited immensely from these treatments. Moreover, the idea that parents wouldn’t have noticed, and in some cases reacted skeptically, to a large surge of kids coming out as trans (which is exactly what we’re seeing by every available metric), as well as the opening of dozens of new gender clinics around the country in a relatively short span, were it not for 4thWaveNow or The Atlantic or [Pick Your Center-Left Bogeyman Du Jour] is, to my mind, delusional.
It doesn’t help the podcast’s credibility that it refers to “watchful waiting,” also known as the Dutch approach, as a form of “conversion therapy” at one point, and at another describes it as simply forcing a trans kid who wants medical intervention to proceed through puberty without it. This is completely incorrect on both fronts — the Dutch approach is obviously not conversion therapy, and the entire point of the protocol is to keep an eye on a kid during childhood with the idea of potentially offering medical intervention not long after the onset of puberty, since the Dutch believed this period can help clarify kids’ gender identities and resolve the question of whether their dysphoria is likely to persist in the long term. Watchful waiting doesn’t really apply to kids who first come out as trans in adolescence, who were much rarer when that protocol was developed.
Elsewhere in the episode, it is explained to listeners that major American medical associations support youth medical transition. This is oversimplified but true to a point, and do you know to what data those organizations point to support their defense of puberty blockers and hormones? The Dutch data, mostly! So this is a very, very confused and conspiratorial podcast produced by folks with radical and under-informed views on the youth transition debates. Not that I’m an unbiased critic, or anything.
We’re gonna have to stage an intervention, aren’t we, Jesse? Stop going to Twitter.
You're very brave for continuing to interact with these people - the transactivists, the journalists (I use the term loosely), and everyone else in this garbage fire. Twitter itself is designed to encourage this type of engagement, which is one reason why I'd be pleased if Elon Musk destroyed it.