

Science-Based Medicine's Coverage Of "Irreversible Damage" Included About 19 Errors, False Claims About Three Sex Researchers, Made-Up Quotes, And Endless Misinformation
There's also an instance of misdemeanor plagiarism

I’m making this article free for everyone, but if you find it useful, please consider becoming a paid subscriber to Singal-Minded or giving a gift subscription:
My paid subscribers are the reason I was able to take such a close, critical look at Science-Based Medicine’s coverage of youth gender medicine. As you will see in parentheticals littered throughout this piece, by the time I published it, SBM had already begun issuing corrections as a result of my work (I tweeted out bits of my findings as I went and emailed the site’s top two editors to see if they wanted to comment). This is similar to the results I garnered after critiquing Science Vs’s and Foreign Policy’s coverage of this same issue. Subpar journalism on this subject is absolutely endemic, and it takes an unfortunate amount of time and effort to debunk it. Thank you for considering becoming a subscriber or gifting a subscription to someone else.
(Update: I switched the title from ‘Includes’ to ‘Included’ to account for the corrections that have been made.)
In my previous article on this subject, I argued that Science-Based Medicine has not lived up to its ideals of rigorous science communication during a recent controversy over Abigail Shrier’s Irreversible Damage: The Transgender Craze Seducing Our Daughters that culminated in the retraction of a positive review by Harriet Hall (reposted here) and a four-part followup series criticizing the book. That article offered an in-depth criticism of the introductory post in SBM’s series, authored by the site’s founder and executive editor, Steven Novella, and its managing editor, David Gorski.
That post also included a lot of important background information that I am not going to repeat here, so if you’re confused, start there. This time around, I’ll be critiquing the middle two of SBM’s four articles in this series: “Abigail Shrier’s Irreversible Damage: A Wealth of Irreversible Misinformation” by Rose Lovell and “Irreversible Damage to the Trans Community: A Critical Review of Abigail Shrier’s Irreversible Damage (Part One)” by AJ Eckert. Part Two of that second post, which I believe will wrap up this series, just went live as I was finishing this article, and for reasons that will soon become apparent, I don’t think I have it in me to respond to that one, though we’ll see.
These middle two articles are not an improvement over Novella and Gorski’s deeply flawed introduction. They include many factual errors that need to be corrected (my rough count is 19 in total), basic misunderstandings and distortions of the scientific literature, glaring omissions that would complicate certain pat narratives, and multiple instances of both authors failing to accurately communicate the content of articles they link to. Lovell and Eckert make demonstrably false, damaging claims about sex researchers, and perhaps worst of all, Eckert includes in their critique of Irreversible Damage references to several quotes that don’t appear anywhere in it — that is, quotes that are made-up (some but not all of which have been corrected). Eckert also commits an admittedly minor act of plagiarism.
(As indicated above, a small subset of these errors have already been corrected, and I am hoping more of them will be after this post goes live. I’m going to refer to both articles in the present tense throughout this post but whenever I reference a false claim that was corrected prior to this article’s publication, I will make that clear in a parenthetical.)
It seems obvious what happened here: At the risk of repeating myself, Science-Based Medicine has abandoned its commitment to rigorous science communication and has decided to wholeheartedly adopt the frequently false and oversimplified claims of activists seeking to derail any conversation or debate about the worrisome holes in the literature on youth gender medicine.
A Critique of “Abigail Shrier’s Irreversible Damage: A Wealth of Irreversible Misinformation”
This one’s authored by Rose Lovell, a doctor who as of February was finishing up her residency. Part of the challenge of responding to Lovell’s article is that she makes many claims in a drive-by manner, without defending them at all. Near the top of her post, for example, she lists “Shrier’s themes and false major claims,” but then never returns to most of them.
One of these supposedly false claims is that “Those who do not embrace the current standards of care [for transgender and gender nonconforming youth] have been unfairly and forcibly removed from their positions (e.g., Kenneth Zucker, Ray Blanchard).” In the course of firing Zucker and shuttering his clinic, the hospital that employed him did, in fact, publicly libel him, as that hospital subsequently acknowledged in a hefty cash settlement accompanied by an apology. Does Lovell disagree with the employer’s own admission? And Ray Blanchard was never removed from a position (as he confirmed to me in an email), so I’m not sure what she’s even referring to here. We never hear anything about either of these incidents again in this article. Science-Based Medicine should correct the false claim that Ray Blanchard was removed from a professional position. You can’t just disseminate false and professionally damaging claims about people you dislike. (In theory, Lovell is referring to claims Shrier made in her book, but nowhere does Shrier say that Blanchard was fired from anything.)
Another “theme and false major claim” of Shrier’s, according to Lovell, is that “The ability of a teenager to know themselves and determine their own course in life is questionable at best.” Lovell offers no clarification here but it appears Science-Based Medicine — a rigorous, evidence-centered website that recently pulled down a book review of Irreversible Damage for not adhering to its scientific standards — is advancing the claim that “The ability of a teenager to know themselves and determine their own course in life is unquestionably sound.” It would be really interesting to hear someone like Lovell lay out this argument in more detail, since it flies in the face of so many decades of developmental psychology research, as well as recent neuroscience findings about how long it takes the human brain to fully develop and how susceptible it is to impulsive and otherwise poor decision-making before it does, but we never hear more. And so on — there are a bunch of instances in which Lovell attributes a supposedly false claim to Shrier but never explains or elaborates.
On at least one occasion, Lovell attempts a strange, cheap potshot at Shrier that distorts the text of Irreversible Damage. She writes that “As for the idea that more young people are seeking services and that more of them were assigned female at birth, that turns out to have some possible basis in data. Not that one could tell from Shrier’s citation of a twitter post referring to the American Society of Plastic Surgeon’s data on gender confirmation surgery statistics[.]”
As is often the case in this series, the writing here is confusing — what does Lovell mean by “Not that one could tell…”? Anyway, this is written in a way that will make SBM readers think Shrier is citing random tweets rather than credible sources. But here’s the full citation in question:
“2017 Plastic Surgery Statistics Report,” American Society of Plastic Surgeons, https://www.plasticsurgery.org/documents/News/Statistics/2017/bodycontouring-gender-confirmation-2017.pdf. This point was made in a fantastic tweet by a mother who goes by the pseudonym “Emma Zane.” EZ, (@ZaneEmma), “Between 2016-2017, the # of sex reassignment surgeries in the US for natal females QUADRUPLED and the ratio flipped, with FTM now accounting for 70% of all SRS (1 year ago it was 46%) This is a public health EPIDEMIC disproportionately affecting young women!” Twitter, November 30, 2018, 4:22 p.m., twitter.com/zaneemma/status/106861616021873868 8?s=12
So Shrier referenced a legitimate statistical report, and then credited a Twitter account for pointing her toward it. It’s unclear what the problem is here. Shrier didn’t ‘cite’ a tweet except to tip her hat to the person who informed her of the report in question.
Going forward, I’ll list some of Lovell’s other claims in bold, indicating that I am quoting her directly, and then respond in normal text.
Where citations are provided for claims – a rare phenomenon in this book! – they usually reference newspaper articles, social media posts (usually Reddit or YouTube), or personal interviews or conversations.
It’s simply false that citations are “a rare phenomenon” in Irreversible Damage. There are endnotes throughout the book, and they point to a Notes section that, in the PDF copy I have, runs from pages 235 to 257. Will any reader who sees this description of citations being ‘rare’ come away thinking there are 22 pages of them in the book? Contrary to Lovell’s claim, Shrier also cites the scientific literature frequently, though also, yes, mainstream news articles, blogs, and so on as well, which makes sense given the context of the book (if you are writing about teen culture, you are going to mention Tumblr and DeviantArt). The book is probably a bit lighter on endnotes than certain other books on scientific controversies, but that’s partly because so much of it is given over to Shrier’s own reporting, and when you’re laying out your own reporting, you are unlikely to include many citations.
This one’s borderline, I suppose, but I do think it’s clear-cut enough that Science-Based Medicine should correct the false claim that citations are “a rare phenomenon” in Irreversible Damage, since no fair-minded reader would describe her citation practices in such terms.
Modern attempts to characterize the population into a simple sex ratio results in an overall estimate of 1:1, as is seen in the US Trans Survey, a population-based survey of transgender and gender non-conforming people in the United States.
This is another good example of how Science-Based Medicine is failing to adhere to its normal scientific standards. Lovell calls the USTS a “population-based survey,” meaning representative of the broader population (that’s how this term and its variants are used in the scientific literature), but all you have to do is read the survey itself to see that the authors caution otherwise:
Although the intention was to recruit a sample that was as representative as possible of transgender people in the U.S., it is important to note that respondents in this study were not randomly sampled and the actual population characteristics of transgender people in the U.S. are not known. Therefore, it is not appropriate to generalize the findings in this study to all transgender people.
Ignoring this caution, Lovell claims that the research found a 1:1 sex ratio among the trans people it surveyed. But this claim is false. The authors report that “More than half (57%) of respondents had female on their original birth certificate, and 43% had male on their original birth certificate. Of those who were non-binary, 80% had female on their original birth certificate, and 20% had male on their original birth certificate.” So no, that is not a 1:1 ratio, and if we were to rely on this as accurate and representative (which we shouldn’t), it would support Shrier’s overall claim of an increase in FtM trans people. (There are arguably backbreaking sampling problems with the USTS that you can read more about here and in this table — it is not good that some influential studies are based on this survey data, including the troubled article on puberty blockers and suicidal ideation by Jack Turban and his colleagues I referenced in my last post and recent Spectator article.)
In summary, Lovell wrote that a non-representative survey which found a skewed sex ratio was a representative survey that found an even sex ratio. (Other than that, this is excellent science communication.) Science-Based Medicine should correct this.
The concern about patients who may change their mind is very old and largely unfounded. One meta-analysis of transgender adults found, at most, a 1% regret rate amongst those who had undergone surgery, including those who had regrets about surgical complications (i.e., unrelated to the transition itself).
It’s unclear why we should see regrets about surgical complications as “unrelated to the transition itself.” Of course the possibility of surgical complications is one factor adults should take into account in determining whether to proceed with such procedures.
On Lovell’s broader point, I addressed this in my last post in some depth: The research on adult regret tells us almost nothing about the question of how to best help transgender youth, particularly those who appear to have later-onset GD. These are just entirely different populations and their healthcare is associated with entirely different bioethical and more general evidentiary considerations. A physician at all familiar with the literature should understand the distinction and recognize the paucity of data on youth gender medicine.
The oft-cited “80% of children will change their mind” statistic comes largely from four observational studies from 2008 to 2013 in Canadian clinics.
Nope. The Zucker clinic in Toronto did not publish four desistance during this time span. Lovell is referring to a mix of studies from the Dutch and Canadian clinics. It’s also not Canadian clinics, plural, but just one clinic — Zucker’s. Again, Lovell just lacks any sort of basic familiarity with this research.
These studies have some significant flaws. The authors included many gender nonconforming children (e.g., male children who like dresses), not just those who verbalized that their gender differed from the sex assigned at birth. That’s actually a huge distinction, as many gender nonconforming children are not and never were transgender. Their sample was flawed to begin with, and they relied on DSM III & IV definitions and diagnostic criteria, which do not match modern understanding.
Lovell is, like Novella and Gorski before her, confused and misinformed about the desistance literature. She repeats the claims that ‘many’ merely gender nonconforming kids were counted as desisters in these studies, going so far as to suggest a male child merely wearing a dress would be enough for him to be treated by these clinicians as gender dysphoric. I explained, at length, why that seems like a stretch in my last post. This is the second consecutive Science-Based Medicine post that claims the DSM-IV criteria were fatally flawed without telling readers exactly what these supposedly inadequate criteria are, or even linking directly to what they say. Can’t have readers evaluating your claims independently by giving them easy access to primary sources.
{kind=link}
The other major criticism of these studies is in the definitions and the follow up. If a participant dropped out of the study they were categorized as “desisters” along with children who no longer were considered to have dysphoria. That clearly was an assumption and artificially inflated the numbers of children who “changed their minds”. Additionally, some studies defined “desisters” using reporting from people other than the participant. It’s also unknown what happened to these young people in their twenties, thirties, or beyond. The studies themselves are behind paywalls, but many criticisms are publicly available.
As written, Lovell is claiming that the Canadian research is hampered by the researchers’ decision to count lost-to-followup patients as ‘desisters.’ But she is, again, confused and unfamiliar with the research, and as a result is leveling yet another false claim — this criticism was made of the Dutch research, most often of a very well-known 2013 study.
Setting that aside, I succumbed to this rumor myself before correcting the record. But if you look closely at the specifics, it just isn’t the case that there were that many kids in this boat, nor that it was an unwarranted belief on the part of the Dutch researchers that lost-to-followup kids were desisters. Of the initially group of dozens of kids who stopped coming to the clinic but who they could get in touch with (either directly or, in a small number of cases, through their parents or guardians — those are the “people other than the participant” in question), either one or zero of them had gender dysphoria, depending on the criteria being used. The Dutch then went ahead and assumed the remaining true lost-to-followup cases, a group about half this size, consisted of desisters as well, in part because there was only one clinic in the Netherlands at which someone could get puberty blockers or hormones. Even if you assume that some of these kids actually did still have gender dysphoria, it wouldn’t change the overall takeaway that desistance was quite common in this sample. No one should hold this study up as providing a precise estimate, as the Dutch researchers themselves have explained, but the idea that they were wildly assuming vast numbers of patients were desisters in an unwarranted, unscientific fashion just isn’t backed by the actual text and methodology of their research.
Again, though: details.
Lovell’s “criticisms are publicly available” line links to the book-chapter version of a 2018 paper published in the International Journal of Transgenderism called “A critical commentary on follow-up studies and ‘desistance’ theories about transgender and gender-nonconforming children.” This paper is often treated as a devastating blow against the desistance literature, but it appears to include basic misunderstandings on multiple fronts, according to two of the Dutch researchers who were criticized in it. They published a response in that same journal titled — naturally — “A critical commentary on ‘A critical commentary on follow-up studies and ‘desistence’ theories about transgender and gender non-conforming children.’”
I’m not going to fully explore that subdebate here since we’ll return to one facet of it in a bit, other than to say the Dutch researchers seem to make some fair points about problems in the other paper. But I simply want to note that the same pattern we saw in SBM’s first post on this subject is maintaining here: SBM acts in a vastly more credulous way toward research pointing in one direction, almost always confidently gainsaying the other’s side’s arguments or counterarguments — or simply ignoring them entirely. The average SBM reader will have no idea that there is (to my mind, at least) genuine controversy over whether the “critical commentary” study was a fair and informed criticism of the desistance literature. This is similar to how, in Novella and Gorski’s post, they mentioned the criticism of Lisa Littman’s work on rapid-onset gender dysphoria but simply ignored the fact that Littman had responded, rather credibly, to some of the most important allegations about it.
But again, it’s apparently important to obscure from readers the idea that there’s any controversy here, since Science-Based Medicine is ideologically committed to the view that the research on youth gender medicine is solid and that any evidence suggesting caution or the possibility of difficult tradeoffs is inherently tainted.
Lastly, as clearly noted in the American Academy of Pediatrics statement, complete with many citations of their own, we use affirmation, pubertal suppression, and hormone therapy in youth because it leads to improved psychological outcomes. The literature is abundant and clear on this topic. Blocking puberty with GnRH agonists is, unlike what Shrier claims, safe and reversible in the pediatric population. Were it not, these medications would not have been in use for decades for precocious puberty.
Knocking an obvious issue out of the way, the fact that puberty blockers “have been in use for decades for precocious puberty” tells us nothing about this very different use-case: The data we have suggest the vast majority of transgender and gender nonconforming (TGNC) kids who go on blockers proceed to cross-sex hormones, and we have almost no longitudinal outcome data on kids who never go through a full natal puberty, but rather a pseudopuberty brought on by exogenous cross-sex hormones. This is very different, for obvious reasons, from putting a kid on blockers, ceasing the blockers, and letting their natural puberty take over. Again, a physician has to understand this. A supposedly rigorous, skeptical science website has to communicate this.
More importantly, it’s pretty inexcusable, in 2021, for a supposedly science-based outlet to describe blockers as “safe and reversible” in such a pat manner. There are now enough questions about this that the U.K.’s National Health Service, for instance, changed its language on this issue from:
The effects of treatment with GnRH analogues are considered to be fully reversible, so treatment can usually be stopped at any time.
To:
Little is known about the long-term side effects of hormone or puberty blockers in children with gender dysphoria.
Although the Gender Identity Development Service (GIDS) advises that is a physically reversible treatment if stopped, it is not known what the psychological effects may be.
It’s also not known whether hormone blockers affect the development of the teenage brain or children’s bones. Side effects may also include hot flushes, fatigue and mood alterations.
Science-Based Medicine is, of course, not required to accept the NHS’s language on this issue. Perhaps there is a parallel universe in which an SBM author lays out the NHS’s concerns, as well as the concerns of others who have raised these issues about the reversibility claim, and explains why they find them to be overblown. That’s what competent, comprehensive scientific communication would look like — even while expressing an opinion of its own, it would fill readers in on an ongoing, pressing controversy.
In our own, endlessly flawed and profoundly exhausting universe, though, Science-Based Medicine readers will have no idea that there even is any controversy on the question of puberty blocker’s reversibility. And that is such a cruel point to deny readers access to, especially given the high likelihood parents trying to figure this stuff out will find their way to this website.
I do think SBM is intentionally bending the evidence to make youth medical transition appear safer and more evidence-based than it is. I know I sound conspiratorial when I say that, but if across multiple articles, all the errors and omissions and oversimplifications invariably point in the same direction, what other conclusion should I arrive at? At a certain point Occam’s razor has to kick in.
As for the “abundant and clear” literature on this topic:
‘Abundant’ links to a study lead-authored by Kristina Olson of young trans kids. Olson and her colleagues recruited parents of trans kids via various venues and gathered some data on their well-being, “examin[ing], for the first time, mental health in a sample of socially transitioned transgender children” by comparing these kids’ mental health to their siblings and some age-and-gender-matched cisgender members of a control group. She and her colleagues found that “Transgender children showed no elevations in depression and slightly elevated anxiety relative to population averages. They did not differ from the control groups on depression symptoms and had only marginally higher anxiety symptoms.”
Because clinical populations of gender dysphoric youth so often have heightened depression and anxiety, some have treted this study as some evidence for the efficacy of social transition. Olson has won a MacArthur grant for her research, and it is indeed important given how little information we have about this population. But as is evident from some of the cautions she and her other colleagues offer in the paper itself, her study wasn’t really designed to assess whether, as Lovell suggests, “affirmation, pubertal suppression, and hormone therapy in youth... leads to improved psychological outcomes.” The short version is that there are simply all sorts of sampling issues and potential confounds in the design that would make this a stretch. It could be the families that volunteered were different from the broader subset of families of gender dysphoric youth, and that these differences account for potentially different outcomes. We also don’t know whether these kids had mental-health problems prior to transitioning, or what would have happened if their parents took more of a Dutch approach and didn’t allow a full social transition, but also didn’t attempt to suppress or pathologize their childrens’ “cross-gender” behavior. These issues don’t render the study moot or unimportant, but they are serious limitations that prevent us from inferring all that much from it.
Whereas other research is picked over for any sign of any flaw — sometimes to the point of inventing flaws that aren’t quite there — this study gets a one-word descriptor and link: ‘abundant.’ My Isolated Demands For Rigor Meter starting smoking and shaking and eventually exploded while I read this, because just one paragraph before approvingly citing this study, Lovell criticized the desistance research for “reporting from people other than the participant.” How did Olson and her colleagues measure these kids’ depression? “Parents completed anxiety and depression measures.” Is this a problem or not? A flaw worth noting or not? As always with SBM’s coverage of this subject, evidentiary standards vary wildly depending on whether the results support the tail that is wagging the coverage.
‘Clear’ links to a study published by a different research group, lead authored by a clinician named Luke Allen. It’s “a longitudinal evaluation of the effectiveness of gender-affirming hormones for improving psychological well-being and decreasing suicidality among transgender youth referred to a transgender health specialty clinic at a large Midwest children’s hospital.” That study did show some apparent improvements in quality of life and suicidal ideation among a cohort of young people who went on hormones for gender dysphoria, albeit over a short followup period and (like basically all of these studies) without any comparator group.
This sounds promising for advocates of youth gender medicine. Remember, though, that key to the Science-Based Medicine ethos is not accepting studies at face value, but critically interrogating their methods and quality. The cofounders of the site say so themselves. Luckily, we have a pair of reviews by the U.K.’s National Institute for Health and Care Excellence, or NICE, evaluating all the research that has been conducted so far on puberty blockers and hormones for TGNC youth.
Less luckily — and fairly remarkably — we’re now two articles and many thousands of words into SBM’s coverage of youth gender medicine and there hasn’t been a single mention of these reviews, nor of similar undertakings by governments organizations in Finland and Sweden. Since all these groups found the same alarming lack of good research for youth gender medicine, and this goes against SBM’s preferred narrative that only dunderheaded bigots have any questions about this field, it’s important for Novella and Gorski, and other authors in this series, to obscure these findings from readers. If you think I’m being uncharitable, can you explain any other situation like this in which a website devoted to communicating medical evidence would ignore these comprehensive reviews in favor of various cherrypicked one-off studies, all pointing in the same direction?
Anyway, NICE mentions the Allen et al study as one of the small handful that appear to show improved outcomes for TGNC youth who go on hormones, but it rates the certainty of the findings as “very low” and the quality of the study as ‘poor,’ in part because of a “high risk of bias (poor quality; lack of blinding and no control group).” This assessment is understandable in light of these and other limitations, such as the failure to control for access to psychotherapy (which might also help reduce suicidality and improve quality of life), plenty of which are mentioned by the researchers themselves when, as is custom, they lay out the limitations of their findings.
To be clear, my point is not that both of these studies should be tossed in the trash. The Olson et al study is valuable because almost no research has been done on the mental health of any cohorts of early-transitioned trans kids. The Allen et al study is valuable because while some research has been done on the outcomes of youth who go on hormones, there’s vanishingly little of it. These studies are both both parts of a puzzle that is (too) slowly being assembled. That’s how science works.
My point is that SBM has completely abandoned its own avowed skepticism and commitment to closely analyzing studies on this one issue, trading in its magnifying glass for pom-poms. Multiple paragraphs are given over to telling us not to trust the desistance literature, and then these studies — very limited in their own findings — are linked to with the assertive, ask-no-question words ‘abundant’ and ‘clear,’ even when one of them suffers from the same flaw that was just mentioned in a much more critical passage.
“Biology is a binary and differences of sex development (DSDs) are vanishingly rare”. False. DSDs are as common as 1 in 5,000 births, and increase to 1 in 200 or 1 in 300 if you include hypospadias and cryptorchidism. Biology is very, very well known to be a spectrum.
In this strange concluding section, Lovell throws out a bunch of what appear to be quotes from Shrier’s book and then attempts to debunk them. These aren’t quotes, though — they’re her own paraphrasing of Shrier’s argument. I do think readers will be confused, but here there’s some ambiguity and I will give her the benefit of the doubt. In the next article, as we’ll see, there’s no doubt that SBM passed along made-up quotes as having come directly from Irreversible Damage.
In this case, Shrier told me she didn’t understand this critique since she doesn’t get into intersex stuff in Irreversible Damage. I emailed Lovell and she mentioned a line that appears to be Shrier’s sole, fleeting reference to this subject. Shrier writes: “Race is a far more trivial biological feature than sex. Unlike male and female—of which there are statistically insignificant abnormal variations— race really does admit a spectrum.” I will try to stop doing all these exasperated asides, I promise, but it is so strange to me that I had to go through a multi-step process, including reaching out to both parties, just to hunt down exactly what Shrier said about this subject so I could evaluate the dueling claims. Why include a paraphrase — in quotes no less! — rather than just quoting her directly? I continue to think the only point here is to obfuscate Shrier’s actual claims and to make her look as silly and reactionary as possible.
Anyway, I don’t think Shrier is using “statistically insignificant” in the traditional, scientific sense — I think she just means something like “very rare.” Or, if she is using it in the traditional sense, the only way to parse her meaning here would be something like “fewer than one in 20 people aren’t straightforwardly male or female,” given that (to oversimplify) that is the mainstream benchmark for “statistical significance.” Either way, Shrier is making the straightforwardly accurate claim that almost everyone is biologically male or female. This is just true, and until recently it was uncontroversial. Even in a 2013 article that in my view bought too much of this spectrum-talk and conflated sex and gender or gender identity in confusing ways, Harriet Hall wrote that “The binary classification is sufficient for most practical purposes and is very useful. In medicine, the knowledge that a patient is male or female helps to guide diagnosis and treatment. We know that men and women have different responses to medications and different incidences of various diseases.”
Lovell fuzzes things up here by attributing to Shrier the difficult-to-parse claim that “biology is a binary.” I don’t know what this means and am going to ignore it, since surely Shrier recognizes that some aspects of biology cannot be conceptualized as binaries — she herself mentions height and race. Her claim, though, is simply that human biological sex is a binary (setting aside a small number of intersex cases), and Lovell offers no real evidence to rebut this view. Were it a spectrum, we’d see a situation where everyone could be placed somewhere on a biological line from “exceptionally female” (one end) to “neither male nor female” (the middle) to “exceptionally male” (the other end). In day to day life, we’d encounter people from all over the spectrum. In this scenario sex would be just like height, where adults can range from three-foot-whatever to almost eight feet tall (with both extremes probably having some sort of medical issue), or race, where people can range from very, very light-skinned to very, very dark-skinned.
Biological sex isn’t anything like that, even if more and more progressives are falling into a pit of ideologically motivated scientific illiteracy on this subject. As Lovell herself notes, when we look for the prevalence of disorders of sex development that might make it difficult to call someone biologically male or female without an asterisk or two, we get something like 1 in 5,000 for more serious variants, or 1 in 200 - 300 for a condition like hypospadias, which is just a birth defect in the genitalia of babies that are clearly, in every way, male. (Everyone should watch Dave, by the way — I’m looking forward to finally diving into Season 2 given how brilliant the first season was.)
In claiming that “Biology is very, very well known to be a spectrum,” Lovell links to a paper which notes that:
The estimated frequency of genital ambiguity is reported to be in the range of 1:2000-1:4500 [1]. According to the Danish Cytogenetic Central Registry, the prevalence of XY females is 6.4 per 100,000 live born females. In this registry, the prevalence of androgen insensitivity was 4.1 per 100,000 live born with median age at diagnosis of 7.5 years. The prevalence of XY gonadal dysgenesis was 1.5 per 100,000 live born females with median age at diagnosis of 17 years [2]. The incidence of DSD varies among ethnic groups with the highest incidence in the southern African population.
Still not a spectrum!
(I should note that in her email to me, Lovell also cited one frequently-mentioned estimate that puts the prevalence of intersex conditions at almost 2%. This figure has been getting batted around forever, but I’m sympathetic to this rebuttal, which argues that the only way to get to such a high figure is to include a number of conditions that would really stretch the definition of ‘intersex,’ since they don’t entail the genuine chromosonal/phenotypal ambiguity we associate with the term. When you leave out those conditions, the estimated prevalence is orders of magnitudes lower.)
“Parents know their children best and have the child’s best interest at heart”. Really? In the United States during 2019, 0.89% of children were reported to be neglected or abused (likely an underestimate due to underreporting), and 77.5% of that neglect and abuse was at the hands of parents. I have seen child abuse in my own practice. It’s not uncommon.
L̶o̶v̶e̶l̶l̶’̶s̶ ̶0̶.̶8̶9̶%̶ ̶r̶a̶t̶e̶ ̶i̶s̶n̶’̶t̶ ̶f̶o̶u̶n̶d̶ ̶a̶n̶y̶w̶h̶e̶r̶e̶ ̶i̶n̶ ̶t̶h̶e̶ ̶r̶e̶p̶o̶r̶t̶ ̶s̶h̶e̶ ̶l̶i̶n̶k̶s̶ ̶t̶o̶ ̶a̶n̶d̶ ̶I̶’̶m̶ ̶n̶o̶t̶ ̶g̶o̶i̶n̶g̶ ̶t̶o̶ ̶t̶r̶y̶ ̶t̶o̶ ̶f̶i̶g̶u̶r̶e̶ ̶o̶u̶t̶ ̶w̶h̶e̶r̶e̶ ̶s̶h̶e̶ ̶g̶o̶t̶ ̶i̶t̶.̶
(Correction, 7/26/2021: I don’t know how I missed this but it says on the third page, “In FFY 2019, an estimated 656,000 children were victims of abuse or neglect nationwide, which is a rate of 8.9 victims per 1,000 children in the population.” That translates, of course, to a rate of 0.89% Lovell’s citation is correct and I apologize for getting this wrong.)
For the sake of argument let’s say this figure isn’t 0.89%, but 5%. Imagine someone saying, “Oh, so you think parents know their children best and have their child’s best interest at heart? Then how do you explain the fact that 5% of them abuse their children?” This is, on its face, a very strange argument. Shrier never claims that there are no abusive parents, of course, but rather is arguing something like, Generally speaking, parents know their kids well enough to understand when they appear to have suddenly developed an interest in transitioning despite a lack of childhood gender dysphoria. Either way, good luck making the argument “Don’t listen to Abigail Shrier — she thinks parents know what is best for their kids” to the normies.
A critique of “Irreversible Damage to the Trans Community: A Critical Review of Abigail Shrier’s book Irreversible Damage (Part One)” by AJ Eckert
Eckert is “Connecticut’s first out non-binary doctor and serves as the Medical Director of Anchor Health’s Gender and Life-Affirming Medicine (GLAM) Program.” Same deal in this section — Eckert’s claims in bold, as direct quotes, followed by my responses.
Throughout her book, Shrier refers to her subjects as “biological girls,” a term that conflates sex with gender and mischaracterizes Shrier’s subjects. The reason is that a person’s sex refers to the identity assigned by doctors, parents, and medical professionals at birth, most often based on external anatomy (genitals). Sex is often confused or interchanged with gender, which involves a person’s own sense of their behaviors, characteristics, thoughts, and social factors, and is not determined by biological sex. A person’s gender may or may not conform to the male and female binary and may or may not align with their sex assigned at birth.
More accurately, Shrier’s subjects are “AFAB”, or “assigned female at birth“, because no one gets to choose what sex they’re assigned at birth. When discussing transgender and gender non-conforming individuals, this terminology is generally preferred over “biological male/female”, “male/female bodied”, “natal male/female”, and “born male/female”, which are considered defamatory and inaccurate.
The term “biological girls” does not “conflate[] sex with gender.” ‘Biological’ is right there, a modifier meant to indicate Shrier is referring to a child’s biological sex rather than gender identity. While the plural form of this phrase doesn’t appear in Irreversible Damage, the singular form appears four times, mostly in the context of Shrier explaining the physical effects of transition and/or her qualms with the so-called “affirming approach” to treating gender dysphoria:
-“No mention is made of the fact that there are no diagnostic or empirical criteria for deciding that a biological girl is in fact ‘really a boy.’” (64)
-“The whole course of appropriate treatment hinges on whether doctors view the patient as a biological girl suffering mental distress or a boy in a girl’s body.” (98)
-“‘[Binding] offered me the ability to shove something that was bothering me to the back of my mind and not have to worry about it,’ said biological-girl-now-trans-man Jackson Tree, according to the article.” (145)
-“If a biological girl regrets her decision and stops taking testosterone, her extra body and facial hair will likely remain, as will her clitoral engorgement, deepened voice, and possibly even the masculinization of her facial features.” (170)
One could argue, on etiquette grounds, that it was rude for Shrier to have referred to Tree’s biological sex — in the vast majority of settings there is no reason to refer to a trans person’s biological sex unless they bring it up. But in three of these four quotes, Shrier is simply using “biological girl” to refer to someone’s biological sex in a setting where it matters a great deal. For Science-Based Medicine to argue that this is inappropriate is surprising.
Or, more accurately, it would have surprised me not too long ago. But SBM is now given over entirely to the activist understanding of this issue, and in that understanding you are not supposed to talk about anyone’s “biological sex,” because biological sex is just too fuzzy a phenomenon to understand or easily categorize — as opposed to gender identity, which despite being a patient’s subjective report of an inherently fuzzy concept, is treated in this model as objectively true in the way we used to view someone’s biological maleness or femaleness as objectively true.
As you can see, Shrier isn’t allowed to use “natal female” or “born female” either, because these are ‘defamatory.’ How is it ‘defamatory’ — that is, “damaging the good reputation of someone; slanderous or libelous” — to call someone a “natal (fe)male”? If you click the link provided in this Science-Based Medicine article, it will take you to what appears to be a basic Word document hosted by New York-Presbyterian hospital and titled “LGBTQ+ Terminology / Vocabulary Primer.” That document simply repeats Eckert’s claim without explaining it at all.
What could this possibly mean? Science-Based Medicine appears to be promoting the view that if a 14-year-old natal female announces they are a trans boy, they are no longer biologically female — after all, it can’t be “considered defamatory and inaccurate” to refer to them as such if the claim is true. If this isn’t what Eckert is saying, what are they saying? This is disturbing, coming from a gender clinician tasked with guiding kids and their families through decisions that can only be made in a truly informed manner if everyone involved has a sophisticated, realistic understanding of biological development and the limits of what puberty blockers and hormones can do. More specifically, you can’t give a child competent care unless they understand they are biologically (fe)male and that this means certain things with regard to what transition will look like, what will happen during puberty if they don’t or de-transition, and so on. (This is an issue the Dutch clinicians mention explicitly in their rundown of their approach.)
Less important but still worth noting, if you actually try to plug the AFAB terminology into Shrier’s claims, it’s readily apparent why it doesn’t work: “If an assigned female at birth teenager regrets her decision and stops taking testosterone, her extra body and facial hair will likely remain, as will her clitoral engorgement, deepened voice, and possibly even the masculinization of her facial features.” This is stilted phrasing that doesn’t really make sense. Those physical changes would set her apart not because she was assigned anything at birth, but because natal females — a class she is a member of regardless of what a doctor says, or her own thoughts on the matter — tend to have much less testosterone, less body and facial hair, and so on. If a doctor had messed up and ‘assigned’ her an M rather than an F, this person would still, in the absence of medical intervention, develop female secondary sex characteristics, menstruate, and so on. There’s nothing ‘assigned’ about any of this. It’s almost like the whole point of these ever-stricter language rules is to make it impossible for any of us to talk about biological realities. But those realities are quite important.
It is also alarming that Science-Based Medicine is not only endorsing but enthusiastically disseminating the view that “a person’s sex refers to the identity assigned by doctors, parents, and medical professionals at birth,” rather than a stable set of physical characteristics that are unambiguous something like more than 99% of the time. Do David Gorski and Steven Novella, longtime critics of bunk scientific claims, themselves endorse this view of what biological sex is? Do they endorse the view that we cannot talk about “biological girls” or “biological females”? If so, they should consider the ramifications this will have for medicine, particularly for women’s healthcare. If not, they should explain how their own views differ and why they think Eckert is wrong. The question of whether or not it is proper, on a website about medical research, to refer to ‘biological’ or ‘natal’ sex, isn’t something that can be tabled — it’s fairly urgent. (Fixed. This paragraph initially read “why they think Lovell is wrong.”)
They won’t explain any of this, of course. Their whole goal here is to keep their heads down, mouth the right pseudoscientific platitudes, and not get in any more of the sort of trouble they got into when they ran a positive review of Irreversible Damage. That’s why they published this series.
(Again, if I’m being uncharitable, explain to me what other theory of their motivations could possibly explain any of this.)
She defends her referring to these subjects using pronouns that do not correctly reflect the gender with which they identify, commonly referred to as “misgendering,” by appealing to the First Amendment, a common strategy employed to attack the rights of LGBTQ people.
This occurs nowhere in the book. At one point Shrier does mention the First Amendment in the context of what she sees as the unconstitutionality of a law that “threatened jail time for healthcare workers who refuse to use patients’ requested gender pronouns,” as well as another one which “applied to employers, landlords, and business owners.” But the brief “Author’s Note” where she explains her stance on pronouns makes no appeal to the First Amendment. Here it is in its entirely:
I take it for granted that teenagers are not quite adults. For the sake of clarity and honesty, I refer to biologically female teens caught up in this transgender craze as “she” and “her.”
Transgender adults are a different matter. I refer to them by the names and pronouns they prefer wherever I can do so without causing confusion.
Finally, I have changed the names and certain minor details of transgender-identifying adolescents (and their parents) to ensure that none is able to recognize herself and accuse her battle-worn parents of treachery. Because the stories of those vulnerable to this contagion are strikingly similar, some readers may believe they have recognized themselves—only to be wrong.
I’m sure some readers will find this offensive and I have my own qualms about how Shrier frames certain aspects of her argument, but the point is that on the factual question of whether Shrier couches her books’s policy about pronouns in First Amendment language, she plainly doesn’t. And it would be weird if she did: She has a law degree and of course understands that her decisions about which pronouns to use in a book have nothing to do with the First Amendment, whereas state laws over how one can refer to others do, at least arguably. Science-Based Medicine should correct this false claim about the content of Irreversible Damage.
The following is Part One of a discussion of the arguments and claims in Shrier’s book and where they go wrong. There is a lot to review here and, as my patients will tell you, I am not one for brevity. I will focus on the core beliefs forming the bedrock of Shrier’s arguments: gender dysphoria in AFAB teenagers is the newest fad; “gender ideology” (or “transgender ideology” or “trans ideology”) pushes teens into “becoming” trans; Rapid Onset Gender Dysphoria is real; the DSM-IV is the superior diagnostic manual because it classified trans identity as a mental illness; 80% of children desist from a trans identity; today’s teens don’t follow the correct rules for being trans and therefore are not trans but definitely are mentally ill.
The DSM-IV did not classify “trans identity” as a mental illness. We’ve already been through this. And Irreversible Damage appears to only mention this older version of the DSM a few times, twice in its reference sections and once in an excerpt in which Shrier notes that transgender identities have recently been normalized — which she couches as an overall good thing:
“Gender dysphoria” still appears in the DSM, but it is already on the way out—no longer called “gender identity disorder,” which emphasized the psychopathology. “Homosexuality” was once classified as a mental disorder, too; most of us no longer believed homosexuality was an impediment to a full and happy life. Maybe appearing in the DSM doesn’t mean anything so bad; maybe it won’t be there for long.
Now, of course Shrier also argues, controversially, that because there’s less and less stigma associated with having GD, an unintended consequence is that teenage girls are turning to it as an explanation for their distress that also brings them some social clout and community. But at no point does Shrier, as SBM suggests, state any sort of preference for one set of diagnostic criteria over the other. I don’t believe she even mentions the specific differences anywhere, other than this fleeting reference to the superficial name change. And of course this is all in a sense moot because we’re talking about a fantasy version of the DSM-IV in which “being trans” is itself a mental disorder. It’s unclear how Shrier even could prefer that version given that it doesn't exist.
Unless I’m missing something and Eckert can provide evidence otherwise, Science-Based Medicine should correct the false claims that the DSM-IV categorizes trans identity as a mental illness and that Abigail Shrier endorsed it over the DSM-5 for that reason.
Shrier also never mentions the 80% desistance statistic. Rather, she pegs this estimate at 70% (weirdly, Eckert acknowledges this further down, so there are mixed messages on this front). And when Shrier does cite this specific figure, it is always in the context of gender dysphoria resolving itself, not a “trans identity” resolving itself. Which makes sense because the studies which lead to this estimate are mostly concerned with the clinical symptoms of gender dysphoria, not the (overlapping but distinct) issue of how a given child identifies.
Here is every mention of this figure in Irreversible Damage, with citations removed:
-“But in most cases—nearly 70 percent—childhood gender dysphoria resolves.” (xxi)
-“Several studies indicate that nearly 70 percent of kids who experience childhood gender dysphoria—and are not affirmed or socially transitioned—eventually outgrow it.” (119)
-“That is a stunning statistic, especially considering that when no intervention is made, roughly 70 percent of children will outgrow gender dysphoria on their own.” (165)
Science-Based Medicine should correct the false claim that Abigail Shrier writes that 80% of kids desist from a trans identity, clarifying that the figure she offers is 70%, and should also clarify that in citing this figure, she is referring to the resolution of gender dysphoria, not a trans identity per se. Eckert knows that these are overlapping but different concepts.
According to Shrier, “before 2012, in fact, there was no scientific literature on girls ages 11-21 ever having developed gender dysphoria at all”. A review of research studies reveals a 1998 research (1) study on puberty delay in trans adolescents, an (2) Introduction to Transmasculine Studies from 2005, 2011 (3) medical guidelines for (4) treatment of transgender youth, and those (5) specific to transmasculine young people, and much more; there is a robust base of scientific literature on AFAB trans youth. One wonders if Shrier knows how to use Google and PubMed, given that these references are not difficult to find. [numbers added by me].
Shrier’s argument is that later-onset youth GD for natal females is a new and lesser-understood phenomenon, whereas researchers have known about both boys and (less often) girls who develop gender dysphoria in earlier childhood for a long time. I think she leaves herself open to criticism with the very bold phrasing here: There was no scientific literature on any kids having developed GD in this age range? It just seems unlikely on its face.
Eckert is certainly skeptical, throwing out not one but five studies supposedly rebutting this claim and then snarkily taking aim at Shrier’s inability to do the most elementary research. Let’s look at these citations one by one:
(1) is a Netherlands case report of a natal female (sorry for the defamation) who “came to the gender clinic requesting sex reassignment surgery at age 16. From interviews with her parents it appeared that she had always been a classical tomboy in her play activities and toy and peer preference and that she wished to be a boy from early on.” This is apparent childhood-onset GD, so it doesn’t debunk Shrier’s claim.
(2) is a paper entitled “The Middle Men: An Introduction to the Transmasculine Identities” that doesn’t appear to have anything to do with the question at hand (“I illuminate the varied experiences of transmasculine individuals by organizing the plethora of defining FTM labels into three broad categories: Woodworkers, Transmen, and Genderqueers”), so it doesn’t appear to debunk Shrier’s claim, either. I do not have it in me to read this 23-page article in its entirety at the moment because my brain already feels like a turtle stranded on its back at noon on a sunny August day in a Brooklyn parking lot, but it is clearly not a scientific report about youth gender dysphoria. If I am wrong and this contains scientific evidence (rather than anecdote) pertaining to natal females developing GD in the 11-21 age range, I will post a correction. I feel like I’m on safe ground here.
(3) is medical guidelines which read, at their very beginning, “Based on the work of Cohen-Kettenis et al in Amsterdam, it is recommended that children with persistent GID and worsening gender dysphoria begin pubertal suppression at Tanner stage 2 after thorough evaluation by a mental health professional that excludes any psychological disorder causing a gender disorder.” The authors also note that “although 80% to 90% of childhood GID desists by adulthood, GID rarely desists after the onset of pubertal development.” These are all references to childhood GID/GD and its persistence/desistance, so nothing here debunks Shrier’s claim.
(4) is a paper on “Management of the Transgender Adolescent” lead-authored by Johanna Olson (now Olson-Kennedy) that barely touches on this specific issue. It does note that “most adolescents and adults with GID report that they experienced cross-gender behavior and identity as children, and many teenagers diagnosed as having GID do have persistence of GID into adulthood. [citations removed].” So while the language of ‘most’ rather than ‘all’ nods to the possibility of later-onset youth GD (including among natal females), this paper offers no information on this population, nor specific references to it. So it doesn’t debunk Shrier’s claim, either.
(5), finally, is a general overview for the assessment and treatment of “Female-to-Male Transgender Adolescents” that, like (4), includes language implicitly nodding at the possibility of later-onset natally female GD youth, but which offers no specific insights or explicit mentions of research on this population. So again, no dice.
For those keeping score, that’s five references to papers supposedly debunking a supposedly laughable scientific claim, none of which actually does debunk that claim. Keeping in mind that the average reader only rarely clicks on links and only super rarely can fully access paywalled research, compare the actual content of these papers to the feeling a paragraph with five links and that snarky remark likely givse to the reader: “Boy, is this woman full of it!” And note how long it can take to debunk false claims, versus how swift a task it must have been for Eckert to lard this paragraph with citations that seemed to be about the question at hand, but which weren’t.
Unless Eckert can point to research suggesting otherwise, Science-Based Medicine should retract its claim that Shrier was wrong to suggest that prior to 2012, there had been on research specific to later-onset youth GD in natal females.
Shrier reports, “for the first time in medical history, natal girls…constitute the majority” (of the “sudden surge of adolescents claiming to have gender dysphoria”). Her cited source examined sex ratios in children and adolescents referred to the Gender Identity Development Service (GIDS) in the UK. The study found an increased ratio of adolescent referrals. Specifically, 32% were AMAB (assigned male at birth); 68% AFAB, which aligned with results from an Amsterdam clinic. However, a Toronto clinic reported a larger proportion of AMAB referrals.
The claim about the Toronto clinic is misleading. If you pull up the linked-to study, you’ll see that it includes the language, “Compared to international data reported by other gender identity clinics, the sex ratio of the child referrals in the UK was more in line with the child sex ratio reported by the Amsterdam clinic (1.25:1, N=860) than with the Toronto clinic, which reported a larger proportion of birth-assigned males referred in childhood.” But Shrier’s argument is about adolescent referrals, as Eckert is clearly aware given that they quote Shrier mentioning this. And mere sentences later in that very same paper: “For adolescents, our findings reflect the general trend of an inversion in sex ratios reported both in Amsterdam and Toronto (in Amsterdam: 1:1.72, N=234; in Toronto: 1:1.76, N=202; Aitken et al., 2015), in the U.S. (1:1.4, N=180; Reisner et al., 2015), and more pronounced in Germany (1:2.9, N =39; Becker, Ravens-Sieberer, Ottová-Jordan, & Schulte-Markwort, 2017) and Finland (1:6.8, N=49; Kaltiala-Heino et al., 2015).” This is fully in line with Shrier’s argument.
In context, this is a false claim — anyone reading this paragraph who doesn’t closely read the paper itself will think the reference is to referral patterns for adolescents at the Toronto clinic. Science-Based Medicine should correct the false claim that the Toronto clinic didn’t see the same natal-sex shift among adolescent patients as other clinics.
The limitations of Shrier’s source are that it draws from anecdotal surveys, small databases, and inconsistent, soft studies, and neglects social/cultural factors, such as the fact that it is often easier for AFAB young people to “come out,” especially since gender-variant behavior in AMAB (assigned male at birth) young people may be more exposing and lead to social stigma. Adolescents not seen at specialized clinics are not represented in gender dysphoria studies, a factor that skews the ratio, therefore, the study can only assume that the data reflects a real change in ratios in the overall trans youth population.
In her references section, Shrier cites multiple gender clinics’ own reports about shifts in referral patterns. What else is she supposed to do? How is a clinic’s own data ‘anecdotal’ or ‘soft’? This is just a strange claim.
[Various school practices mostly pertaining to LGBT activism and education that Shrier doesn’t like] are characterized as a “woke gender ideology,” an oft-recited phrase that is never really defined.
I don’t think Eckert really read this book. At least not closely. Far from being “oft-recited,” The phrase “woke gender ideology” appears nowhere in it. Science-Based Medicine should correct this claim and clarify that the phrase never appears in Irreversible damage. (This was corrected before this article went live — see Error #2.)
According to Shrier, the internet coaches and indoctrinates teenagers in “radical trans ideology” (again, whatever that means).
The phrase “radical trans ideology” appears nowhere in Irreversible Damage. Science-Based Medicine should correct this claim and clarify that the phrase never appears in the book. (This was corrected before this article went live — see Error #3.)
[Lisa] Littman speculated that ROGD could be a “social coping mechanism” for other disorders. Her study was published in 2018 and pulled shortly thereafter, a move described by Shrier as “activists stormed the peer-reviewed scientific journal accusing her of anti-trans bigotry”. Littman’s study deliberately skewed results by drawing from blogs openly hostile to transgender youth, the same blogswhereLittman developed the concept of ROGD in the first place. The study formed its conclusions around the beliefs of parents who already presupposed the existence of ROGD, since Littman only posted her survey on the three blogs that invented and promoted ROGD. Today, the entire research base of ROGD consists of one 2017 poster abstract of an online survey of 164 parents.
This timeline is false, as Littman confirmed to me. Eckert is apparently confused. Faced with political pressure, Brown university pulled a press release about the study. Littman’s study itself was never ‘pulled’ from anything. Rather, as a result of the political pressure PLOS One published an updated version and a ‘correction’ that noted none of the results had changed. As I mentioned in my previous post, the journal also confirmed to me that the correction was not made in reaction to any factual inaccuracies:

Similar to the Ray Blanchard issue above, this is a damaging false claim about a sex researcher. Littman’s paper was never retracted. Science-Based Medicine should correct the false claim that Littman’s study was ‘pulled,’ as well as the related false claim that “the entire research base of ROGD” consists of one poster. (The ‘pulled’ claim was corrected before I published this article — see Error #4.)
As is par for the course here, the linking is also confusing — that final claim about the poster includes two links that critique Littman’s research, but neither of which makes any mention of a ‘poster’ or the number 164. In the absence of accurate linking and citing, it’s effectively impossible to fact-check Eckerts’ claims.
Judging by the attitudes of parents surveyed, I would posit that their children were likely afraid to disclose due to minority stress factors including social stigma, fears of rejection, and very real concerns about violence.
Science-Based Medicine is accusing a bunch of parents it doesn’t know of likely being physically abusive toward their kids, because they are skeptical their kids should go on blockers and/or hormones. Is this Eckert’s approach, in their own practice, to the inevitable disagreement that sometimes arises between parents and teens when it comes to hormones and blockers? Do they believe that when a parent has qualms about these treatments, that means they are at a high risk of physically assaulting their children? How does that affect the way they go about their job?
Shrier identifies a “real” transgender person as one for whom “the body feels wrong,” and for whom “the only option is to present as the opposite sex.” She states that “they want to pass.”
The quotes about “the body feels wrong” and “the only option is to present as the opposite sex” appear nowhere in Irreversible Damage. Science-Based Medicine should issue a correction listing these quotes and clarifying that they never appear in the book.
There is one mention of people who “want to ‘pass’,” but Shrier is not describing them as ‘real’ trans people and contrasting them with (I guess) ‘fake’ ones. Here is the full passage in question:
This book is not about transgender adults, though in the course of writing it I interviewed many—those who present as women and those who present as men. They are kind, thoughtful, and decent. They describe the relentless chafe of a body that feels all wrong, that seems somehow a lie. It is a feeling that has dogged them for as long as they can remember.
Their dysphoria certainly never made them popular; more often than not, it was a source of unease and embarrassment. Growing up, none of them knew a single other trans person, and the internet did not yet exist to supply mentors. But they didn’t want or need mentors: they knew how they felt. Presenting as the opposite sex simply makes them more comfortable. They do not seek to be celebrated for the life they have chosen. They want to “pass”—and, in many cases, to be left alone.
For what it’s worth, Shrier said in a Twitter direct message, “I never talk about who is and isn't ‘really trans’ -- again, I don't even know what that means.” Now, the book does posit that some kids who think that they have gender dysphoria, and that therefore they should transition, aren’t actually gender dysphoric, but are misinterpreting other sources of distress as gender dysphoria. So I could understand how someone could claim, in general sense, that part of Irreversible Damage is about the idea of some people not ‘really’ being trans. But the version Eckert lays out, in which Shrier says something like People who A, B, and C are really trans, but people who X, Y, and Y aren’t. doesn’t seem to appear anywhere. Unless Eckert can provide some evidence otherwise, Science-Based Medicine should correct this claim.
It is important to Shrier that we know that gender dysphoria was previously known as Gender Identity Disorder. She uses an outdated version of the DSM manual, DSM-IV, and conflates gender dysphoria with gender identity disorder to define it as characterized by a severe and persistent discomfort in one’s biological sex. … By citing the DSM-IV, Shrier establishes her reality where being transgender is a pathology to be fixed.
The chronic lack of accurate direct quoting from Irreversible Damage initially made this difficult for me to decode, but I think Eckert is criticizing Shrier for writing that “[g]ender dysphoria—formerly known as ‘gender identity disorder’— is characterized by a severe and persistent discomfort in one’s biological sex” (xxi). Eckert claims this is from the DSM-IV, and sure enough Shrier cites it here when she introduces the concept of gender dysphoria (not sure why). But wait — I thought the DSM-IV, according to Eckert, erred in claiming that merely being trans was a mental disorder, rather than the more visceral, harmful feeling of genuine gender dysphoria. They seem to be backtracking, because of course “a severe and persistent discomfort in one’s biological sex” is not a definition for “being trans” (not all trans people have gender dysphoria), but rather a definition of GD. Eckert cannot keep straight which diagnostic criteria they are critiquing and why
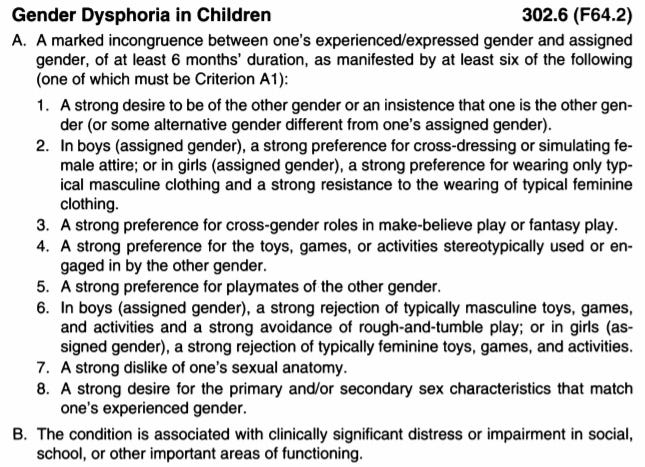
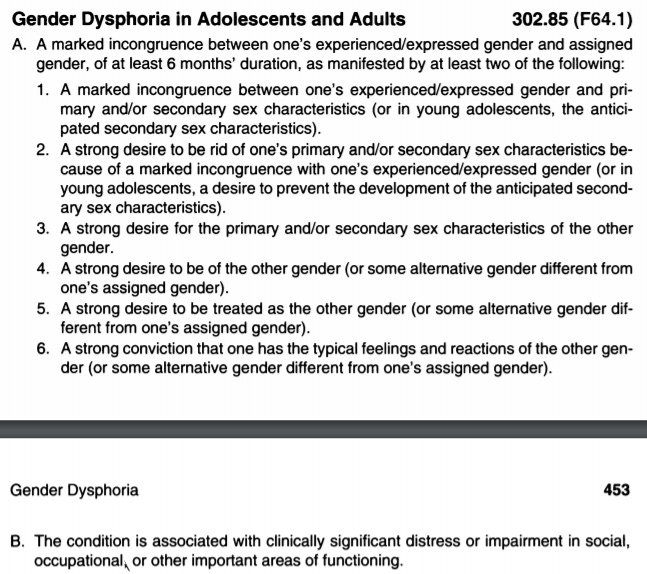
Anyway, if you go to the DSM-5’s GD entries for both kids and adolescents and adults (more details here), in both cases the first sentence reads “A marked incongruence between one’s experienced/expressed gender and assigned gender, of at least 6 months’ duration, as manifested by…,” followed by the criteria for each category. This is almost identical to “a severe and persistent discomfort in one’s biological sex” — it’s just a matter of “biological sex” having been swapped out for “assigned gender” for the purposes of preventing the DSM-5 from getting thrown violently off the euphemism treadmill (by 2040, “assigned sex/gender” will be considered offensive). If someone asked me to define “gender dysphoria,” I’d do so similarly to how Shrier does, because I think “biological sex” is a perfectly fine term to use. There’s just nothing wrong with her definition at all and it’s effectively identical to the DSM-5’s.
{kind=link}
{kind=link}
We’ve already been over the myth that there is some profound difference between the DSM-IV and the DSM-5, and here Eckert is inadvertently exposing that as a myth. And again, there’s just nothing in Irreversible Damage to suggest that Shrier is relying on outdated criteria in any way that would matter, except to the extent that, like anyone citing the desistance literature, she is forced to rely on some studies that used the DSM-IV. But she gives no indication she favors it, and as we’ve already seen it’s only barely mentioned at all.
These statements belie Shrier’s understanding of being trans as a mental health disorder, despite medical consensus that variations in gender expression represent normal dimensions of human development, and the removal of gender identity disorder from the DSM nearly 20 years ago.
I don’t know how many times I can repeat this, but a disorder corresponding to gender dysphoria was not ‘removed’ from the DSM in any sense. Rather, the name of the condition in question was changed from “gender identity disorder” to “gender dysphoria” and the criteria refined. It is still a disorder. It seems impossible to me that Eckert, a practicing clinician, doesn't know this.
Some linguistic slipperiness is right out in the open here: Eckert is treating “variations in gender expression,” which of course are a “normal dimension of human development,” as interchangeable with “gender dysphoria,” which causes people such intense distress they often seek out serious, permanent medical treatments, and which is considered by the DSM to be a mental disorder. Shrier doesn’t claim “being trans” is a mental disorder — as she pointed out to me and notes explicitly in the book, she has met plenty of trans people who live happy lives and who suffer none of the anguish we associate with mental disorders. This is actually a perfect example of the potential utility and clarity of treating GD as a mental disorder: If you transition and your GD symptoms abate, you no longer have a mental disorder, or at least not an active one, because merely “being trans” does not on its own entail anguish in the way gender dysphoria does. These distinctions matter a great deal, and Science-Based Medicine should correct this false claim about Irreversible Damage.
The belief that a diagnosis is clinically required to access gender affirming care, known as transmedicalism, can contribute to stigma and discrimination toward transgender individuals. Gender dysphoria is not a requirement of being trans[.]
This is concerning. Science-Based Medicine is platforming a youth gender clinician who is disseminating the idea that it is bad to require a clinical diagnosis prior to the administration of puberty blockers and hormones to young people. Again: What does this person’s practice in Connecticut look like?
And less important, but more of that slipperiness! The second sentence has nothing to do with the first. The “requirement[s] of being trans” is a totally different tissue from the requirements for going on hormones. Trans people are the people the trans community accepts as trans — it’s an interesting sociological issue but is completely irrelevant to the controversies surrounding the prescription of hormones and blockers to kids. (This lack of terminological clarity and consistency and coherence is a chronic issue in this debate, so to be clear Eckert is far from the only offender.)
Shrier writes that gender dysphoria resolves in 70% of children who identify as trans. This statement sees her confusing two separate claims. The 70% statistic comes from Dr. Kenneth Zucker, who stated that a full 70% of the children he saw at his clinic for treatment did not have gender dysphoria in the first place.
It’s Eckert who is confused. Their link, to a commentary by Zucker, does not support this claim — in fact, in the commentary Zucker quotes a 2008 study he coauthored in which he and his colleagues wrote that “40% of the girls were not judged to have met the complete DSM criteria for GID,” meaning 60% did. Again, this is just a noteworthy level of sloppiness and misinformation: Eckert claims that Zucker said X, linking, as evidence, to a study in which he cites himself (and others) saying almost the exact opposite of X. Very unusual for a generally credible science website.
So why does Eckert think 70% of the kids at this clinic were subthreshold for GID, anyway? Probably because this is a rumor that has been floating around for half a decade. In my 2016 article on the shuttering of Zucker’s clinic, I wrote:
[The External Review used to justify the closing] simply does not read, at any point, like a serious attempt to evaluate the Gender Identity Clinic, and it is riddled with sloppiness. From very early on, there are simple errors — CAMH’s legal counsel is described as “Kristen Sharpe” four times in the document, when her actual name is Kristin Taylor, and the reviewers note that the clinic has been around for “approximately 30 years” when it was actually founded more than 40 years ago, in 1975. More importantly, Zinck and Pignatiello quote Zucker as stating that “70% of the children we see are sub-threshold for [gender dysphoria].” Whether Zucker misspoke or the authors mistranscribed, this is exactly backwards — 70 percent of the children at the GIC did meet the clinical criteria for the condition (a statistic mentioned in [a] 2008 article and confirmed to me by former GIC clinicians). If the reviewers believed that just 30 percent of them met the criteria — they didn’t respond to an email about this — that would imply they fundamentally misunderstood what the clinic did and why it was treating most of its patients at all.
Eckert could have easily double-checked this with Zucker. I did. “Completely inaccurate,” he said of Eckert’s claim via email. “The particulars can be found in the attached papers.” One is about natal girls (that’s the one he quotes in the commentary), one is on natal boys, and the third is… the commentary itself. You know, the same one Eckert uses to claim Zucker said the thing that is the opposite of what he said. In both the research papers, 60% or more of the kids had what was then GID. How many times, now, has Eckert been unsuccessful at the basic task of reading a paper and accurately communicating its findings to the SBM audience?
Science-Based Medicine should correct the false claims that 70% of the kids in Zucker’s clinic didn’t meet the threshold for a diagnosis of GID, and that Zucker himself said so.
The original studies [on desistance] used the (at the time current) diagnostic criteria of Gender Identity Disorder in the DSM-IV, which were predominately focused on gender expression, meaning that cisgender children, such as AFAB “tomboys” and AMAB boys who liked to play with feminine-coded toys, and other children with gender non-conforming behaviors, were included in the GID category.
I think this is a misreading of the DSM-IV criteria. I’m tired of pasting these criteria in so many posts but here you go (and they appear to be reproduced in searchable text form here):

The very first phrase is “a strong and persistent cross-gender identification.” Of course ‘identification’ is different from ‘expression.’ Yes, some of the criteria have to do with expression. That is part of how you diagnose gender dysphoria/gender identity disorder, especially in kids. But it’s just false that these criteria were ‘predominately’ about gender expression, in my view.
And remember that the DSM-IV also included language that directly contradicts Eckert’s claim that tomboys (for example) “were included in the GID category”:
Gender Identity Disorder can be distinguished from simple nonconformity to stereotypical sex role behavior by the extent and pervasiveness of the cross-gender wishes, interests, and activities. This disorder is not meant to describe a child's nonconformity to stereotypic sex-role behavior as, for example, in “tomboyishness” in girls or “sissyish” behavior in boys. Rather, it represents a profound disturbance of the individual's sense of identity with regard to maleness or femaleness. Behavior in children that merely does not fit the cultural stereotype of masculinity or femininity should not be given the diagnosis unless the full syndrome is present, including marked distress or impairment. [emphasis in the original]
So we have:
Eckert: “AFAB ‘tomboys’ and AMAB boys who liked to play with feminine-coded toys, and other children with gender non-conforming behaviors, were included in the GID category [in the DSM-IV].”
The DSM-IV itself: “This disorder is not meant to describe a child's nonconformity to stereotypic sex-role behavior as, for example, in ‘tomboyishness’ in girls or ‘sissyish’ behavior in boys.”
Science-Based Medicine should correct this.
Research was limited to those children whose parents brought them to the clinic for diagnosis and treatment, believing that their child’s identity was a problem requiring psychiatric treatment.
Here Eckert appears to be cribbing directly from the authors of that “A critical commentary on follow-up studies and ‘desistance’ theories about transgender and gender-nonconforming children” paper mentioned earlier. And I mean very directly. In that paper, the authors write, “Furthermore, even within Toronto and the Netherlands, this research was limited to children whose parents chose to bring them to a clinic for diagnosis and treatment and thus may have believed the child’s difference was a problem, and one that required psychological treatment.” Setting aside the minor plagiarism issue (minor given that Eckert only steals part of one sentence, but to be clear this is plagiarism, albeit of the misdemeanor variety in which a traditional outlet would rush up an explanation that it was just a matter of a forgotten links or quotes or both), it’s worth noting the aforementioned response piece from the Dutch clinicians themselves:
[T]he two remaining [desistance] studies [being discussed] come from two clinics with very different social contexts. The Toronto and Amsterdam clinical populations are not similar. This is illustrated clearly by a number of comparative studies on the social and emotional functioning of children and adolescents who are referred to the two clinics: in all studies psychological functioning in children and adolescents (measured through parental, teacher and/or self-report) showed to be better in Amsterdam than in Toronto (Cohen-Kettenis, Owen, Kaijser, & Bradley, 2003; de Vries, Steensma, VanderLaan, Cohen-Kettenis, & Zucker, 2016; Steensma et al., 2014). As noted in the discussions of these papers, we believe that differences in the social climate regarding gender variance may be an important factor underlying the differences. A sociometric study on peer group status (Wallien, Veentra, Kreukels, & Cohen-Kettenis, 2010) underscores this point. It was shown that there were no differences between gender-referred elementary school children and their classmates in victimization or bullying. Parents who come to our clinic are concerned about potential harm for their child if they would not acknowledge the child's gender experience. They are not focused on suppressing it, as the authors suggest by the sentence: [The sentence I quoted above.]
Again, rumor and innuendo that appear to undermine the desistance literature is passed off as fact over and over and over and over by Science-Based Medicine, as if by compulsion. SBM is not required to accept, as true, the Dutch clinician’s claims about the nature of the parents they saw. But at the same time, it’s obviously unfair for the site to state, as a fact, that the desistance “[r]esearch was limited to those children whose parents brought them to the clinic for diagnosis and treatment, believing that their child’s identity was a problem requiring psychiatric treatment,” and to not explain to readers that the Dutch clinicians themselves — the clinicians who invented the very idea of a medical treatment for pubescent trans youth and who had firsthand experience with all these parents — vehemently deny the claim. You’ll note the only substantive change Eckert makes to the sentence they are cribbing, other than changing “psychological treatment” to “psychiatric treatment” is taking out the slightly hedge-y “may have believed” language to make the overall claim stronger, to make it sound like these studies only involved intolerant parents.
Science-Based Medicine should correct the much too strong, false claim that these studies were only conducted on kids who parents brought them into gender clinics because they believed their very identities required psychiatric treatment, and should correct and address this minor instance of plagiarism.
The four clinics had high ratios of participants who did not follow up: 22%, 25%, 30%, and 32%. Lack of re-engagement with the clinic, for whatever reason, was counted as desistance.
At first I didn’t know where these numbers come from because of the total absence of links or citations. But Eckert’s cribbed sentence led me to a table in that “critical commentary” that has these figures:

Eckert seems to think this research comes from four different clinics (it doesn’t — it comes from two), and is over-extending a critique of one (the Dutch, who did count nonresponders as desisters) to another (I don’t think anyone has ever even made this claim about the Toronto clinic, and when I asked Zucker he said no one had). This is backed up by this chart (which I can’t vouch for and am not going to fact-check at the moment — see earlier parking-lot comment), which suggests the one study included from the Canadian clinic did not count nonresponders as desisters.
Science-Based Medicine should correct the false claim that all four studies had this feature.
In 2003, the American Academy of Child and Adolescent Psychiatry (AACAP) reported that Zucker practiced “something disturbingly close to reparative therapy for homosexuals”.
This description of the AACAP’s supposed findings is inaccurate. A single letter published in a journal run by the AACAP made this claim. That is obviously a far cry from a professional body coming to this conclusion officially, which is what anyone who read Eckert’s article will come away believing is what happened. The difference between “a letter published in a medical body’s journal” and “the official opinion of a medical body” is not subtle, and anyone with a basic familiarity with this sort of publishing would have grokked this distinction. Again, Eckert displays a complete inability to accurately convey the results of published articles to the Science-Based Medicine audience. (This was corrected before I published this article: See Error #1.)
[I]nvestigators reviewed his patient files and found that 72% of the children treated by Zucker never met the clinical criteria for gender dysphoria[.]
Again, no links. Readers will have no idea where this came from. I guess that’s the point. Science-Based Medicine should correct this and make it clear that while the investigators did ‘report’ this, they were false to have done so. All of the clinics’ published research suggests 60% or more of its patients had what was then called gender identity disorder, depending on the subsample in questions. And the external report in question isn’t even available online anymore — the hospital yanked it offline when it recognized the defamation issues, never to re-publish it (though it did throw up a shorter Executive Summary). Say it with me: Science-Based Medicine doesn’t care how shoddy a source is as long as it supports the site’s priors on youth gender medicine.
Zucker ascribed to outdated and harmful conversion therapy practices, and following provincial legislation outlawing gender identity change efforts, his clinic was shut down.
To repeat, Zucker was later given more than a half a million Canadian dollars after his hospital acknowledged having libelled him during a demonstrably haphazard and sloppy ‘review.’ Of course SBM readers arriving to this controversy fresh will have no way of knowing that. It’s journalistically inexcusable to, in two consecutive articles in this series, simply leave out this fact. Now, does this fact, on its own, exculpate Zucker? Of course it doesn’t. But you can’t say “This guy was fired from his job!” without adding the very relevant followup “…and then his employer admitted to having done him wrong and paid him half a million dollars.” It’s just off-the-charts dishonesty by omission.
And again: All the omissions, across multiple SBM articles, point in one direction. Zucker is one of Shrier’s sources and is treated credibly by her, so SBM readers need to know he is Bad, with zero countervailing evidence allowed in. The same pattern, over and over and over. Can’t be an accident.
Countering this narrative, a cross-sectional study of 27,715 U.S. trans adults found that recalled exposure to gender identity conversion efforts was significantly associated with severe psychological distress in the previous month and lifetime suicide efforts. Those exposed to gender identity conversion efforts before age 10 had a significantly increased risk of lifetime suicide attempts.
Surely genuine conversion therapy is harmful, but here we have another example of Science-Based Medicine passing on flawed research in a completely credulous manner. This is another Turban study, based on that same troubled dataset, and there are serious questions about its methodology and whether it is capturing exposure to actual conversion therapy. This post has already ballooned to an unmanageable length, so I’ll just leave this link here, let people decide for themselves, and call attention, one final time, to how SBM treats studies that point in one direction on the youth gender medicine debate versus how it treats those pointing the other way.
I think that while all three of these articles were quite shoddy and communicated a great deal of misinformation, Eckert’s was the most eye-popping. The above is a very partial list of the problems with it. On a couple different occasions, I considered critiquing other half-truths and questionable claims from it, but I need to wrap this up so I’ll cut myself off here. At present count, this post has catalogued what I would argue are 19 errors that should be corrected across the Lovell and Eckert articles, the vast majority of them from the latter, and only a small handful of which have been corrected so far.
People of good faith will surely differ on how many of these errors are serious enough, or objectively false enough, to warrant correction. And in some cases the issues I’m raising are surely genuine errors, but surely minor ones (saying four studies had a given alleged flaw when just three of them did, for example). I do not think people of good faith can differ on the question of whether these articles, along with the introduction to the series penned by Gorski and Novella, meet Science-Based Medicine’s own explicitly stated standards. Of course they don’t. Not even close.
In a way, the most disturbing part of this whole episode occurred at the very end. I wrote most of this post on Sunday. Early Saturday evening, I emailed Gorski and Novella to give them a heads-up that I was working on something accusing their website of having published made-up quotes, and seeing if they wanted to comment. I linked to some of the tweets I’d done on all this as I researched, and also mentioned the false claims about Littman (her study being pulled) and Zucker (that 70% non-threshold zombie statistic).
On Sunday, Gorski and Novella, or Eckert, or whoever is presently controlling Eckert’s post, issued some corrections addressing my concerns — still a long way to go on that front, and they have thus far ignored the issue with the 70% statistic. But Gorski and Novella also published Eckert’s Part Two. This might not come across as shocking if you don’t have an editorial background, but it is! If I commissioned someone to write a two-part series about an author and her book, and then Part One included multiple made-up quotes, I would sure as hell put Part Two on hold as soon as I found out, if only to investigate, make sure there weren’t other issues, etc. To simply throw up Part Two without looking into these issues is well outside the bounds of normal editorial oversight. I’m not saying they should have never published it, but maybe a brief pause for a modicum of heretofore absent quality control? And contrast this with Novella and Gorski’s treatment of Harriet Hall’s review, which never did anything as serious or wrong as making up quotes. That one had to be fully retracted.
It isn’t a mystery what’s going on here, and I really think Science-Based Medicine has flown entirely off the rails on this subject.
Questions? Comments? I usually put a joke here but I’m so very tired? I’m at singalminded@gmail.com or on Twitter at @jessesingal. The main image, the Science-Based Logo with the tagline “Exploring issues & controversies in science & medicine” underneath, is from the SBM website.
This is a nice, long, science-based and very detailed post with plenty of references... just the sort of thing that SBM used to publish.
Joking aside, they've published a lot of posts on quackery, which is a good thing because a naturopath treating cancer with turmeric is going to kill people. A lot of their pieces are basically polemics, which is rather defensible when you're writing about stuff like cupping, where there really isn't a good argument for the practice. But polemics don't really work that well when the evidence is not clear-cut, and they often publish polemics where the evidence isn't clear. I've noticed that in some cases, the pieces tend to fall into the category of "destroying" something and then overstate the evidence or insist that there's no ambiguity when there most certainly is. If that's your site's general tone, chances are that your authors will take the same approach for stuff where the science isn't clear, but the author has strong opinions.
It's unfortunate, because overall, it means that people will question the articles on the site that are strongly grounded in science.
Hrm, saw this elsewhere, not sure if if changes the point but you say "Lovell’s 0.89% rate isn’t found anywhere in the report she links to and I’m not going to try to figure out where she got it." but it seems like the ".89" percent of children abused is pretty clearly on page 2 of that report: "Approximately one-fifth (16.7 percent) of the children investigated were found
to be victims of abuse or neglect—a rate of 8.9 per 1,000 children in the population." https://www.childwelfare.gov/pubPDFs/canstats.pdf