

The University of Washington Is Putting Trans Kids At Risk By Distorting Suicide Research
This has been a shameful episode

I’m only able to do the work I do because of my paying subscribers. If you find this useful, please consider becoming one or giving a gift subscription.
Anyone who has read my work knows that I am not a fan of harm inflation. I don’t like the tendency to treat more and more things as “harmful” or even “violent,” because I think this is usually a derailing tactic employed by individuals who don’t want to engage in conversation or argument.
But it’s obviously true that in some cases, the propagation of some types of information can be reasonably described as harmful or even potentially dangerous. Few of even the free-speechiest of free speech bros would deny this. And I genuinely think what the University of Washington School of Medicine is doing — has been doing, since April — could put trans kids at risk.
For those late to this: In April I published a very long post laying out the severe flaws in a study about puberty blockers and hormones University of Washington researchers published in JAMA Network Open, and how they exaggerated the results when describing them to the media and to UW’s own PR apparatus. The very short version is that the study has so many flaws that it does not provide us with any evidence whatsoever supporting the idea that kids who went on gender-affirming medicine (GAM) experienced beneficial outcomes relative to the kids who did not.
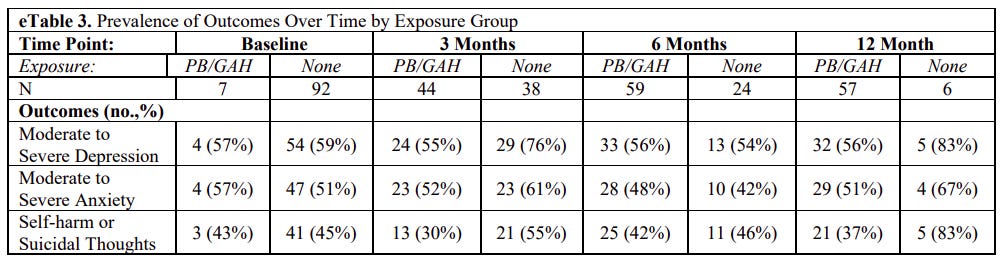
In fact, any genuine comparison between the GAM and no-GAM kids 12 months out is impossible, because 80% of the kids who didn’t go on GAM had dropped out of the study by the final wave of data collection, leaving just six remaining. That is far too small a sample to draw any conclusions from. (The paper gave no explanation as to why some kids went on GAM and others didn’t, making it impossible to know whether this was an otherwise apples-to-apples comparison, so even in the absence of this attrition issue, the results would have been difficult to interpret.)
Moreover, the researchers employed an unusual statistical technique that, according to one of the leading experts on said technique, was ill-suited to the task at hand. Both this and the researchers’ other methodological and editorial choices all pointed in the same direction: exaggerating their results and obscuring the specifics that could have helped third parties determine whether they really found what they claimed to have found. The data they did present were extremely crude and hard to parse — despite having passed peer review, this was not a professionally conducted or written study.
Both the paper and the supplementary materials suffered from a notable dearth of very basic statistical information. When I initially reached out to the lead author, Diana Tordoff, then a PhD student in the epidemiology department at UW, she said she and her team were sharing the data for transparency’s sake. When I pointed out that, in fact, the data was not available where it should be, she stopped responding. “Jesse, contacted the team, and they have no further comment at this time,” said a PR person when I followed up. “They decided to let the methods section speak for itself.”
As a result of my work and inquiries, UW slightly walked back some of its PR claims, particularly language about how depression and/or suicidality had “dropped” or “plummeted” in kids who went on GAM, when the researchers’ own supplemental table appears to show those kids didn’t meaningfully improve over the course of the study.
But this didn’t do anything to address the many misleading claims UW’s researchers and PR apparatus seeded the media with, which spread widely among liberal-minded consumers of science information eager for empirical ammunition in the fight against right-wing efforts to ban or heavily restrict youth gender medicine.
Then, last month, Jason Rantz, a conservative radio host and journalist based in Seattle, published a follow-up story that includes internal UW emails he obtained as a result of a public records request. These emails really highlight the degree to which the comms staff didn’t care whether and to what extent false information about youth suicide was spread by their institution — all they cared about was that most of the media coverage had been positive. It was a victory, as far as they were concerned, and because the outlets sending them inquiries after my story went up were all conservative, they didn’t see any need to respond substantively. (I should note that Rantz’s piece initially contained some inadvertent misinformation of its own, I think, concerning an email from a UW PR staffer that read in part: “UW Epidemiology/UW SPH/UW News will not be including this article in our media tracking/or otherwise driving traffic to this piece.” Rantz interpreted “this article” as meaning the Tordoff et al. study itself, but I think in context it’s almost certainly a reference to my article. It wouldn’t really make sense for a PR person to make this sort of a stand, whereas it would make sense for them to choose not to draw traffic to negative coverage. Rantz at least updated his article with my interpretation.)
I’m a little bit worried that in my last post, despite its “very, very long” length (as an internal UW person described it), I wasn’t sufficiently clear on one point: It’s not just that we can’t say the GAM kids improved, and that we can’t say that they did better than the no-GAM kids. We also can’t say the no-GAM kids worsened. This isn’t much more accurate than the original claim of the kids who received treatment experiencing “plummeting” rates of depression and suicide.
Just to be clear, because there were 92 kids in the no-treatment group at baseline, and just six left at the 12-month mark…
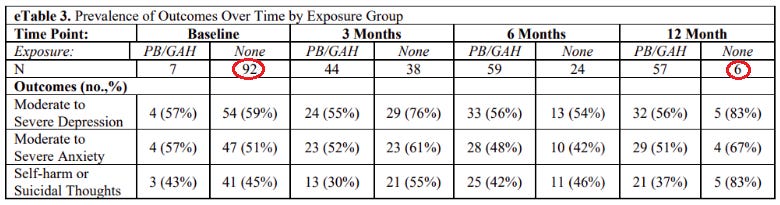
…WE KNOW APPROXIMATELY NOTHING ABOUT HOW THE NO-TREATMENT KIDS WERE DOING 12 MONTHS LATER.
Apologies for the gratuitous over-formatting, but I honestly have felt like I’ve been taking crazy pills watching both UW and, in some cases, scientists with actual credentials defend the claim that we know anything about how the no-treatment kids fared 12 months later. We don’t. It’s literally right there in the chart! Sure, the authors did almost everything they could to hide the fact that the vast majority of their no-treatment kids were lost to follow-up by brushing it under the rug (that is, hiding it in the supplemental material) and not mentioning it in the paper itself, but it is, on its own, a major problem that dictates we cannot draw any meaningful 12-month conclusions about the effects of GAM versus no-GAM in this cohort. It’s as simple as that. There is no way to circumvent this reality, even if the researchers made a strained attempt to do so by employing an ill-fitting statistical technique to elide the fact that they have no (sorry, sorry) useful 12-month comparison data (again, refer to my article, and particularly the quotes from generalized estimating equations expert James Hanley, for more information).
If this exact data and methodology were being used to defend the claim that Muslims are more likely to be terrorists, or that vegetarians are more likely to be weaklings, or any other conservative-coded claim, the internet’s ever-growing ranks of debunkers, fact-checkers, and anti-misinformation experts would be all over it like ants on a discarded scoop of ice cream. But because these fake results point in the direction liberals want, liberals at worst offered ridiculously off-base defenses of this research — in effect coming to the aid of truly shoddy researchers who don’t deserve third-party defenders, given the lackluster quality of their work — and at best stuck their heads deep in the sand, pretending that there isn’t something disturbing going on here.
But the way the team behind this study promoted it was unconscionably misleading. The worst offender was Arin Collin, a UW medical student. During a late February podcast interview, she said the following:
I really appreciate the opportunity to speak about this. This is particularly important because at baseline, transgender youth just experience such disproportionately adverse mental health outcomes. This is due to a combination of factors — we have social exclusion, but also lack of access to medical care. So as an example, we had a cohort here of 100. For total youth and the baseline of outcomes, there were 56.7% of them had moderate to severe depression, 50% anxiety, and 43.4%, at the start of the study, had some level of suicidality, meaning suicidal thoughts or as much as self-harm. What our study found was just vast reductions in depression and suicidality, a reduction of depression of 60%, suicidality 73%. More to the point, we also saw worsening of these, as much as two- to three-fold and severity for the folks who did not receive similar care.
…
We don't see these sorts of improvements with any sort of other treatment.
She made a similar claim in an interview with the outlet Crosscut: “Also, for the folks who did not receive this care, the severity of the depression itself was much worse.”
Everything about this is ridiculous if you simply read the study. The only two real possibilities are that Collin, dispatched by UW to talk up these results, was not familiar with what her research team had actually found, in which case of course she shouldn’t be discussing them publicly. Another is that she is intentionally misleading the public.
In addition, as I noted in my original post, Collin touted the study on Reddit, with the title “Transgender and nonbinary youth who received gender affirming medical care experienced greatly reduced rates of suicidality and depression over the course of 12 months.”
In a follow-up email to UW I wrote late last month, I asked: “Given that Collin appeared to be speaking as a representative of UW in these interviews and the Reddit post, with her affiliation mentioned in all of them, has there been any attempt to contact these outlets and get them to run corrections or clarifications, or to remove the Reddit post, which has around 13,500 upvotes?”
No response to that, though at some point between then and now Collin deleted the Reddit post with, apparently, no explanation — or at least I’m not seeing any on Reddit:

My original article went up on April 6. It took about five months — and a follow-up nudge from me — for Collin and/or her university to decide this plainly inaccurate post needed to come down. Of course, by the time it was deleted, the news had spread far and wide, all of it beneficial to UW (as they note in the emails Rantz got). What’s a little bit of misinformation about youth suicide in exchange for enhancing your university’s stature?
I also asked the PR folks: “More broadly, is the University of Washington concerned with the potential ethical implications of its communications approach here? It seems possible that given how far and wide this study has spread, and given how many UW sources have confidently claimed this study showed reduced suicide rates among the kids who went on blockers and hormones, parents will wrongly believe that these blockers and hormones significantly ameliorate suicidality, which could lead to terrible results.”
Again, no response.
Here’s the one question they did respond to: “At the 12-month mark, there were only 6 kids left in the no-treatment group, since 80% of that group had dropped out of the study. By the normal standards of statistical science, this means that it’s impossible to say much of anything about how the no-treatment group fared over 12 months. Given that UW has repeatedly advertised that this research offers informative results about how kids who didn’t go on blockers or hormones fared after 12 months, do UW and/or the authors disagree with this argument about the attrition rate?”
The response I received suggested that the researchers (who are telling the PR folks how to respond to these inquiries) either genuinely do not understand the very basic question I’m asking, or think that I’m extremely bad at my job. The PR contact wrote back to say that the “findings did not change when the data were analyzed in multiple different ways. This included a supplemental analysis omitting the final (12 month) timepoint at which fewer youth responded due to the fact that this timepoint was added late, and youth had to be recontacted to ask if they wanted to participate.” My entire argument is that the team has almost no 12-month data allowing for a genuine comparison in the first place. To say “Well, when we threw out the data we do have, we got the same result” is borderline nonsensical. (Collin wrote a follow-up post on Reddit that is a version of this statement and that offers the same non-response.)
Anyway, there’s still a press release up touting these findings. It’s walked back but still contains exaggerated bloviation. “Gender-affirming care is lifesaving care,” Collin says in it. “This care does have a great deal of power in walking back baseline adverse mental-health outcomes that the transgender population overwhelmingly [experiences] at a very young age.” There is simply nothing in the study she coauthored to justify these claims. This is a really bad breach of ethical science communications. You cannot publish these results and then tout your intervention as “lifesaving.” It’s insane to me that other members of the medical establishment believe this to be acceptable, but they’re silent about this, which means UW gets queries only from conservatives, which means the university thinks it can keep spreading potentially dangerous nonsense.
I’m also confused as to why no one sees a potential conflict of interest here. The study took place at Seattle Children’s Hospital, two of the authors are based there (almost all of the others are at other UW institutions), and it “was supported [by] Seattle Children’s Center for Diversity and Health Equity and the Pacific Hospital Preservation Development Authority.” Seattle Children’s Hospital has a gender clinic. You don’t need to be a conspiracy theorist to see that a given hospital and its gender clinic benefit, rather straightforwardly, from the claim that the treatments offered there have lifesaving benefits. There’s nothing wrong with gender clinics publishing data, and in fact far more of them should. But to inaccurately portray that data in a manner that has the effect of advertising your clinic’s services misleadingly… again, how is this okay?
Perhaps hundreds of thousands of people believe that the UW School of Medicine found that puberty blockers and hormones had a profoundly salutary effect on the mental health of trans youth, including reducing the probability they will kill themselves, because the University of Washington and the researchers behind this study banded together to flood the zone with exactly this misleading message in a coordinated, highly polished PR campaign.
As I noted in my query to the university, this could lead to terrible or even tragic results. Trans kids often have other complex mental health problems in addition to their gender concerns, and if parents operate under the misperception that there’s a recent, powerful study that found that GAM alone alleviates these problems, it could lead to a blinkered approach to a given child’s care. It’s genuinely dangerous — I am comfortable using this term here — to spread misinformation about adolescent suicide, whatever the specifics. This whole episode has been a shameful instance of hyperpoliticized pseudoscience winning out over critical inquiry and scientific rigor — and on an incredibly fraught, high-stakes subject.
Questions? Comments? Harmful words? I’m at singalminded@gmail.com or on Twitter at @jessesingal. The photograph from the UW campus comes from here.
One thing that sticks in my mind about this issue is the implicit blackmail. "Your kid will kill themselves if you don't do X!" is a jarring and terrifying framework for any parent to deal with, but I'm not aware of it existing anywhere in healthcare except in trans issues.
Consider for example if my teenager told me they'd kill themselves if they're not allowed to watch TV. MAYBE unlimited TV is the only way to ensure they don't carry out their threat, but if so this only reveals a deeply dysfunctional mindset that should be further investigated.
This inquiry seems to be completely missing from the trans discourse as far as I can tell. I find it genuinely alarming how little curiosity there is from the trans-affirming side as to *what* exactly causes someone to be feel dysphoria. The inquiry almost doesn't seem to matter, with the prognosis basically taking the form of "don't worry about why, just make sure they get cutting-edge plastic surgery and experimental hormonal treatments or else they'll kill themselves."
The current state of "gender affirming care" seems like a band-aid solution that papers over a much deeper problem, and I don't understand how we are helping trans people by turning a blind eye to the root cause of their suffering.
I think Dolly put it well here: https://bprice.substack.com/p/lots-of-kids-have-real-and-diagnosable
Jesse, this is such great work! As someone who can (barely) make sense of statistical data included in scientific papers, I know that it takes careful, detailed analysis to document the flaws. I admire your ability and commitment to doing so and applaud your perseverance. Thank you!!!